

|
You need to know most (but not all) of the material on this page. The Exam won't ask you a question directly about Kroenke et al.. Instead, you'll be asked about "a Contemporary Study in clinical psychology other than Carlsson et al." or perhaps "a Contemporary Study into a disorder other than schizophrenia". You won't get asked specifically about what's in the PHQ or Kroenke's sample or anything like that.
|

|
KROENKE ET AL. (2008)
| ||||
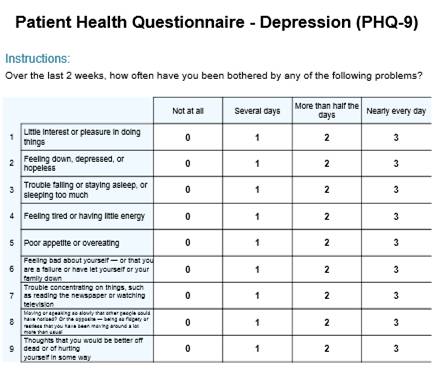
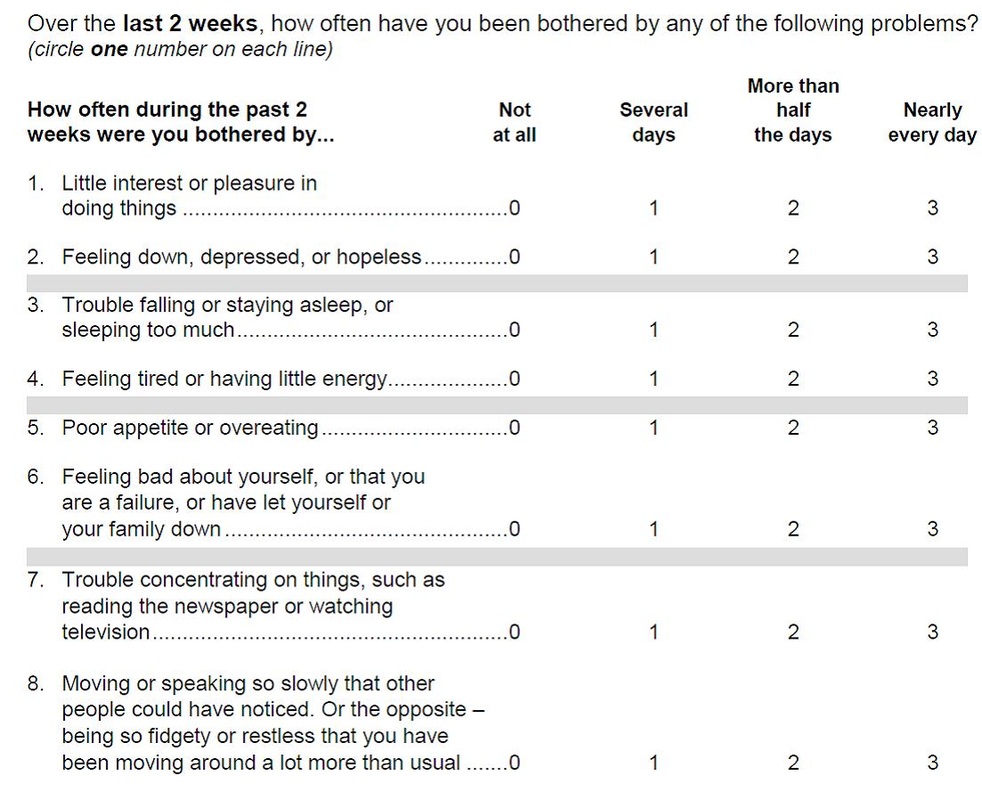
The link up above is to PHQ-9, suicidal thoughts and everything. These downloads are PHQ-8, as used in this study.
|
| ||
The PHQ does a bit more than just indicate how severe a person's depression is. It also seems to make a fairly accurate diagnosis of clinical (unipolar) depression. In particular, if the respondent scores 10 or more on PHQ, that indicates a depressive disorder (as proposed by Kroenke et al., 2001).
The question is, is the score of ≥ 10 on PHQ a reliable and valid way of diagnosing someone with a depressive disorder?
The question is, is the score of ≥ 10 on PHQ a reliable and valid way of diagnosing someone with a depressive disorder?
|
KROENKE ET AL.'S STUDY
|
|
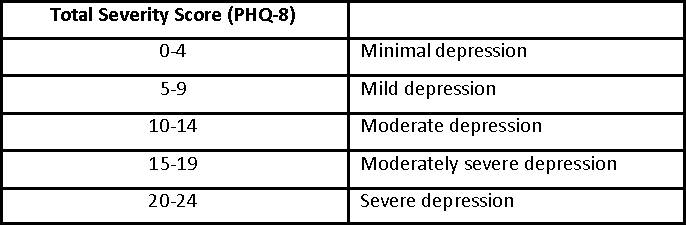
Kroenke et al. used the same categories as the PHQ-9, but adapted them to the new 8-qustion scale. Based on previous research (Kroenke et al., 2001), PHQ-8 cutpoint ≥10 is a good indicator of clinical depression.
|
|
9.1% of respondents were judged to have a depressive disorder based on the PHQ algorithm; 8.6% scored ≥10 on PHQ-8.
According to DSM-IV, out of the 17,040 respondents with a PHQ-8 score > 10, major depressive disorder (MDD) was present in 49.7%, other depressive disorders in 23.9% and depressed mood or anhedonia in another 22.8%. In only 3.5% was there no evidence of depressive disorder or depressive symptoms according to DSM-IV.
According to DSM-IV, out of the 17,040 respondents with a PHQ-8 score > 10, major depressive disorder (MDD) was present in 49.7%, other depressive disorders in 23.9% and depressed mood or anhedonia in another 22.8%. In only 3.5% was there no evidence of depressive disorder or depressive symptoms according to DSM-IV.
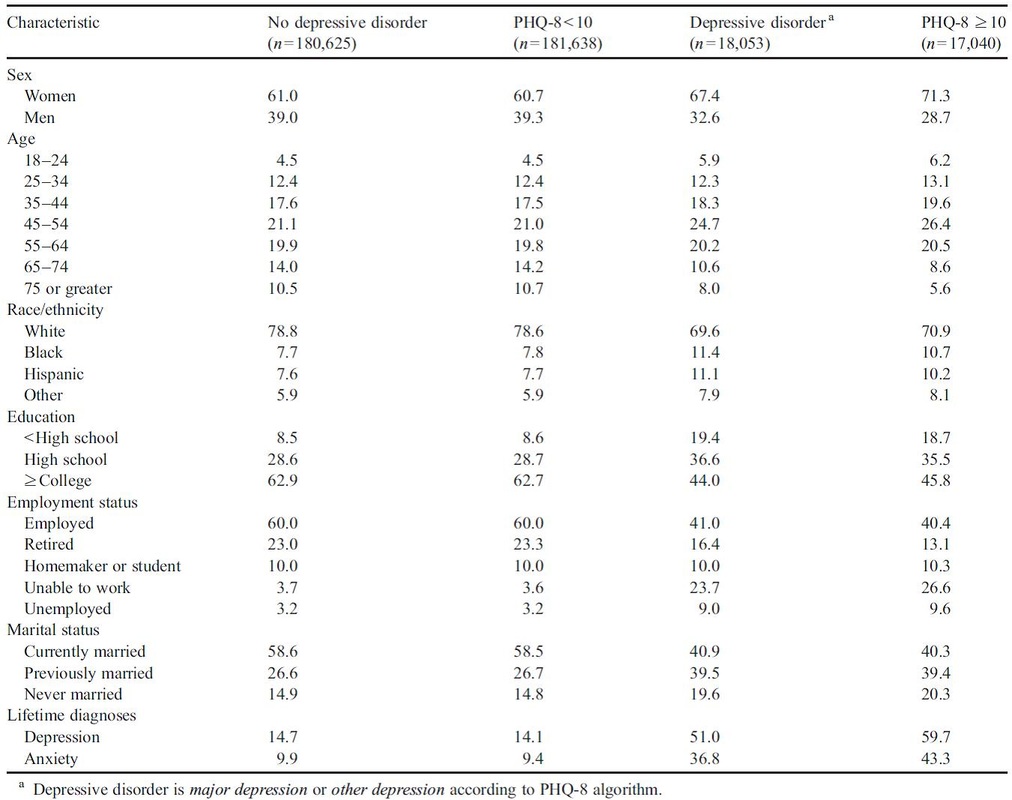
There's a lot of data here but you don't need much of it. Just notice how similar all the percentages are for depressive disorder (DSM-IV-based algorithm) and PHQ-8 score > 10. Pick two particular examples to use in the Exam - like "previously married" people who are almost identical and "retired" people, where there's a bigger gap.
Some of this data might be useful for you to answer questions on individual differences in mental health. Look at the difference between men and women and the "spike" in the 45-54 age group .
Some of this data might be useful for you to answer questions on individual differences in mental health. Look at the difference between men and women and the "spike" in the 45-54 age group .
|
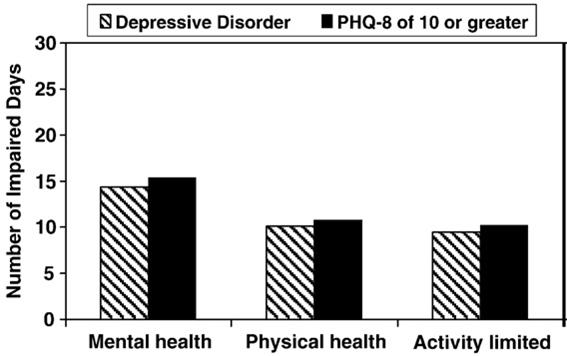
Respondents classified as depressed had more days of impairment on all 3 mental health questions.
This was nearly identical whichever way depression was diagnosed (depressive disorder according to algorithm or PHQ-8 cutpoint ≥10). |
Conclusions
The PHQ-8 is a useful depression measure for population-based studies. Its cutpoint ≥10 can be used for diagnosing depression.
The PHQ-8 is a useful depression measure for population-based studies. Its cutpoint ≥10 can be used for diagnosing depression.

|
EVALUATING KROENKE ET AL. AO3
|

Don't start with description: start with evaluation.
Evaluation point + evidence = "logical chain of reasoning"
4 of these "logical chains" are enough for a 8-mark question
Issues & Debates make great conclusions
|
EXEMPLAR ESSAY
|