
|
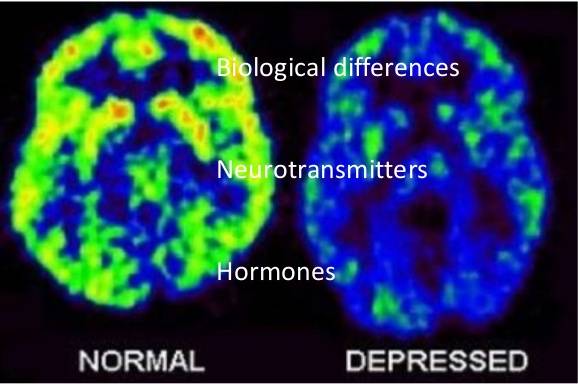
BIOLOGICAL EXPLANATIONS OF DEPRESSION
The Unit 2 Exam expects you to know about one biological explanation of a disorder other than schizophrenia: here, unipolar depression.
You are also expected to understand a biological treatment for depression which is linked to these explanations. There's a strong biological link with depression, which seems to run in families. Elliot Gershon (1990) reviewed 10 family studies and found that the rate of depression was 2-3 times higher in first degree relatives of people with depression (their parents, siblings and children) compared to the general population.
|

|
DEPRESSION & THE FUNCTIONS OF NEUROTRANSMITTERS
|
|
Among the monoamines, serotonin is particularly important. One of its jobs is to regulate the other neurotransmitters. Without the regulation provided by serotonin, brain functioning becomes erratic.
|
|
High levels of serotonin would boost noradrenaline and dopamine, producing a hyper-alert and psychotic state of mind. This is linked to another condition called bipolar disorder - also known as manic-depression.
|
Depressed mood states can be caused by low levels of noradrenaline or dopamine, but the main culprit is the serotonin, which is controlling the other two. A particular gene called 5-HTT has been linked to regulating serotonin levels. People with variations of the 5-HTT gene that are under-active seem more likely to suffer depression after stressful life events.
Rosenthal's diathesis-stress model explains that a gene that produces a mental disorder can be "triggered" by a stressful environment. |
However, the problem might not be low levels of the neurotransmitters themselves. It might be a problem with the receptors that pick up the neurotransmitters when they cross the synapse from one neuron to another. If there aren't enough receptors - or if the receptors aren't working properly - this will have the same effect as a lack of the neurotransmitter.
|
Research focuses on a chemical called monoamine oxidase A (MAO-A), which is a chemical that removes monoamines from the synapse. This is an important brain function called "re-uptake" that recycles neurotransmitters when they don't appear to be needed.
However, if there is too much MAO-A in the synapse, it will remove monoamines that are needed, starving the brain of serotonin, noradrenaline and dopamine, leading to symptoms of depression. This is the basis for a lot of antidepressant drugs, which inhibit (reduce) the activity of MAO-A. This leads to more monoamine activity and a reduction in the symptoms of depression. |
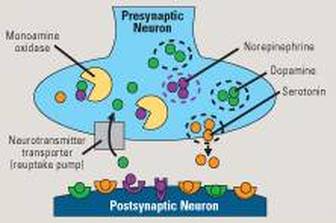
The MAO-A is like "Pac Man", gobbling up excess monoamines. Now imagine Pac Man out of control!
|
You can compare this to the "synaptic pruning" explanation for schizophrenia. In both cases, a normal healthy process in the brain goes too far, producing unhealthy results.
MAO-A is also linked to aggression. When MAO-A levels are too LOW, people experience violent impulses (Brunner et al., 1993)
MAO-A is also linked to aggression. When MAO-A levels are too LOW, people experience violent impulses (Brunner et al., 1993)
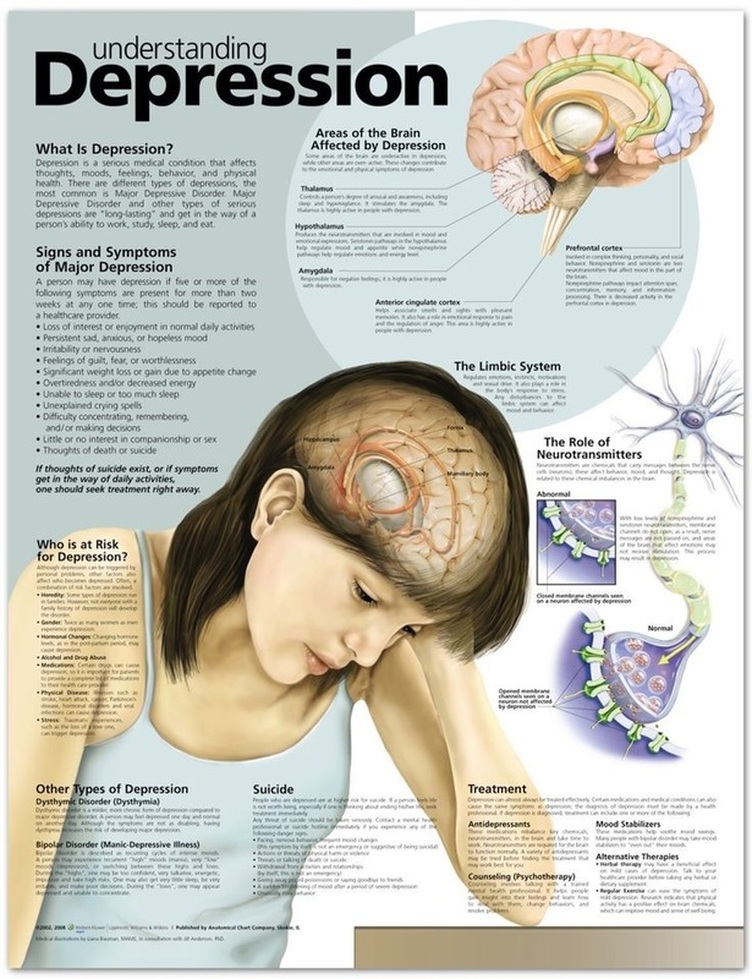
Fantastic poster that covers features and symptoms of depression as well as biological explanations

|
APPLYING BIOLOGICAL EXPLANATIONS OF DEPRESSION
|
|
EVALUATING BIOLOGICAL EXPLANATIONS
|
|
|
EXEMPLAR ESSAY
|