

|
BIOLOGICAL TREATMENTS FOR SCHIZOPHRENIA
The Edexcel course requires you to know about one biologically-based treatment for schizophrenia. You will need to be able to compare this with a psychological treatment.
There are other biological treatments besides drug therapy. For example, there is shock therapy (electro-convulsive therapy or ECT) and psychosurgery (like the frontal lobotomy procedure) but these are uncommon (and unethical) in 21st century medicine.
|

|
DRUG THERAPY SCHIZOPHRENIA
|
|
Because these side-effects are unpleasant, it's difficult to keep patients on their medication once they are released from hospital.
The more serious side-effects are even nastier:
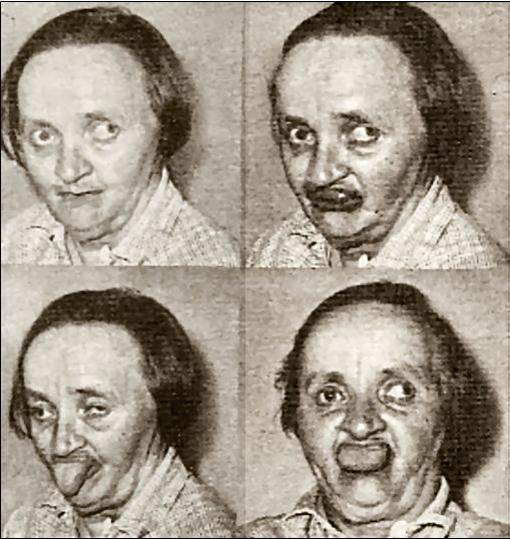
Patients on PTZ often developed a distinctive stumbling walk which was called "the Thorazine shuffle". The worst side-effect is tardive dyskinesia (TD), which causes uncontrollable facial grimaces and tics. TD affects 25% of all patients who take PTZ for more than 7 years. TD is often irreversible even if the patient stops taking the drugs. |
|
ATYPICAL ANTIPSYCHOTICS
The first second-generation, or atypical antipsychotic (AAP) drug was clozapine, which appeared in 1971. Risperidone followed in 1993 and olanzapine in the 2000s.
AAPs do not necessarily work by blocking dopamine receptors - clozapine blocks serotonin instead. This means that scientists are not entirely sure why they have the therapeutic effects that they do. They are more powerful than typical antipsychotics and are usually prescribed as a "last resort" or for people for whom the side-effects of PTZ are too severe.
AAPs benefit 85% of patients with schizophrenia, compared with 65% given PTZ (Awad & Voruganti, 1999). Meltzer (1999) found that a third of patients who had shown no improvement with PTZ responded well to clozapine. Moreover, AAPs do treat the negative symptoms as well as positive symptoms (Remington & Kapur, 2000).
It was hoped that AAPs would not have the same side-effects as PTZ. The second generation drugs seemed to have fewer side effects like dry mouth, constipation and TD. In fact, AAPs produce their own side-effects, like diabetes. TD is a possible side-effect with AAPs as well, but onset takes longer (decades). AAps also seem to produce withdrawal effects which increase the symptoms of schizophrenia, so it's important to come off such medication slowly.
AAPs do not necessarily work by blocking dopamine receptors - clozapine blocks serotonin instead. This means that scientists are not entirely sure why they have the therapeutic effects that they do. They are more powerful than typical antipsychotics and are usually prescribed as a "last resort" or for people for whom the side-effects of PTZ are too severe.
AAPs benefit 85% of patients with schizophrenia, compared with 65% given PTZ (Awad & Voruganti, 1999). Meltzer (1999) found that a third of patients who had shown no improvement with PTZ responded well to clozapine. Moreover, AAPs do treat the negative symptoms as well as positive symptoms (Remington & Kapur, 2000).
It was hoped that AAPs would not have the same side-effects as PTZ. The second generation drugs seemed to have fewer side effects like dry mouth, constipation and TD. In fact, AAPs produce their own side-effects, like diabetes. TD is a possible side-effect with AAPs as well, but onset takes longer (decades). AAps also seem to produce withdrawal effects which increase the symptoms of schizophrenia, so it's important to come off such medication slowly.
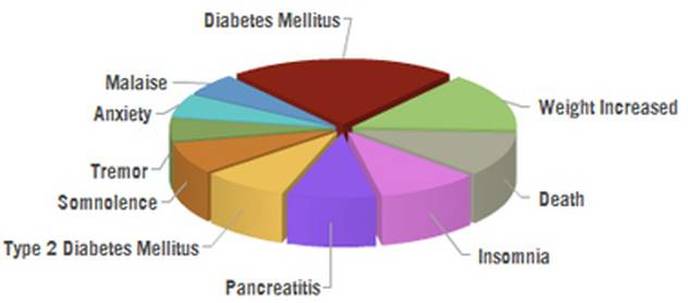
Adverse reactions (side-effects) to all types of antipsychotic: "malaise" is general discomfort; "pancreatitis" is inflammation of the pancreas; TD would fall under "tremor"

|
APPLYING DRUG THERAPY TO REAL LIFE
|
|
EVALUATING DRUG THERAPY
|
|
Some critics argue that antipsychotics are a "placebo" - they only work because the patient believes they will work. This was tested by Meltzer et al. (2014) who used 481 patients with schizophrenia. The patients were put in 3 conditions: (1) patients receiving one of four new trial drugs; (2) patients receiving a typical antipsychotic (haloperidol); (3) patients receiving a placebo (a pill that looked like an antipsychotic but had no effect).
|
|
After 6 weeks, patients taking haloperidol and two of the trial drugs had reduced symptoms. Patients taking the placebo and two of the other trial drugs were still the same. This shows that antipsychotics do better than placebos and really do reduce symptoms.
Drug therapy is supported by the Dopamine Hypothesis and lends support to the biological explanation of schizophrenia. All antipsychotics affect neurotransmitters in the brain to bring about changes in symptoms. When an idea is backed up by a well-researched scientific theory, it has construct validity.
Drug therapy is supported by the Dopamine Hypothesis and lends support to the biological explanation of schizophrenia. All antipsychotics affect neurotransmitters in the brain to bring about changes in symptoms. When an idea is backed up by a well-researched scientific theory, it has construct validity.
Objections
Drug therapy doesn't work for everyone. Although more patients respond to the atypical drugs than to the first generation antipsychotics, this is still not all patients. It is estimated 50-65% of patients benefit from drug treatments.
The main weakness of drug therapy is that it isn’t a cure, it just temporarily reduces the symptoms; as soon as the patient stops taking them, the symptoms return, usually within 3-6 weeks. The first generation antipsychotics were criticised for being a "chemical straitjacket" that turned patients into shuffling, drooling zombies. There are issues of social control here: drugs might be prescribed, not because they help the patient, but because they make the patient easier for hospital staff to control.
Drug therapy doesn't work for everyone. Although more patients respond to the atypical drugs than to the first generation antipsychotics, this is still not all patients. It is estimated 50-65% of patients benefit from drug treatments.
The main weakness of drug therapy is that it isn’t a cure, it just temporarily reduces the symptoms; as soon as the patient stops taking them, the symptoms return, usually within 3-6 weeks. The first generation antipsychotics were criticised for being a "chemical straitjacket" that turned patients into shuffling, drooling zombies. There are issues of social control here: drugs might be prescribed, not because they help the patient, but because they make the patient easier for hospital staff to control.
The classic film One Flew Over The Cuckoo's Nest (1975) shows how the hospital staff hand out medication to control the patients and keep them docile and obedient
All the drugs used to treat schizophrenia have adverse reactions; these could include weight gain, tremors and drowsiness. Some people feel the side-effects are worse than the symptoms they are alleviating. The Recovery Model takes a different approach, urging people with schizophrenia to stop taking drugs and find different ways of living with their symptoms. Harlow et al. (2012) carried out a 20-year longitudinal study and found that patients who did not take their medication had fewer psychotic episodes than those who did.
The Recovery Movement makes some good points but also advocates a lot of conspiracy theories, like the idea that the medical drugs companies ("Big Pharma") deliberately push expensive AAPs onto people to boost their own profits.
Nonetheless, there is a growing concern that antipsychotics are being over-prescribed:
Nonetheless, there is a growing concern that antipsychotics are being over-prescribed:
For some people, remaining on medication long-term might impede a full return to wellness. For others, discontinuing medication can be disastrous - Thomas Insel
Differences
The alternative treatment we are considering is cognitive behavioural therapy (CBT)
CBT used to be considered inappropriate for schizophrenia because cognitive therapy involves talking and thinking clearly - exactly what schizophrenia interferes with. However, Bradshaw (1998) challenged this with a case study that showed a patient (Carol) benefiting from CBT.
The great advantage of CBT over drug therapy is the lack of side-effects. On the other hand, cognitive therapy can be more threatening for some patients, because you have to open up and talk about your problems. For some people, popping a pill is preferable to sharing unpleasant thoughts and feelings with a therapist.
Both treatments take time to be effective: drug therapy takes days-to-weeks, cognitive therapy takes months. This means a patient who is very distressed and perhaps suicidal will get much more help in the short term from antipsychotics.
However, in the long term, CBT might be more beneficial. Carol showed that the benefits of CBT were still there a year after the therapy ended. Whereas, the longer someone takes antipsychotics, the more likely severe side-effects will develop and, if they stop taking the drugs, their symptoms will return.
CBT seems to be most effective with clients who have good problem solving skills. For this reason it has not been seen as appropriate for psychotic patients (Ellis, 1980). However recent studies (Kingdon and Turkington, 1994) suggest that, in combination with anti-psychotic drugs, CBT can reduce delusions and disturbing hallucinations (through reality testing). An "integrated approach" involves combining the two treatments. It may be possible to reduce the dependency on antipsychotics as the cognitive therapy takes effect.
The great advantage of CBT over drug therapy is the lack of side-effects. On the other hand, cognitive therapy can be more threatening for some patients, because you have to open up and talk about your problems. For some people, popping a pill is preferable to sharing unpleasant thoughts and feelings with a therapist.
Both treatments take time to be effective: drug therapy takes days-to-weeks, cognitive therapy takes months. This means a patient who is very distressed and perhaps suicidal will get much more help in the short term from antipsychotics.
However, in the long term, CBT might be more beneficial. Carol showed that the benefits of CBT were still there a year after the therapy ended. Whereas, the longer someone takes antipsychotics, the more likely severe side-effects will develop and, if they stop taking the drugs, their symptoms will return.
CBT seems to be most effective with clients who have good problem solving skills. For this reason it has not been seen as appropriate for psychotic patients (Ellis, 1980). However recent studies (Kingdon and Turkington, 1994) suggest that, in combination with anti-psychotic drugs, CBT can reduce delusions and disturbing hallucinations (through reality testing). An "integrated approach" involves combining the two treatments. It may be possible to reduce the dependency on antipsychotics as the cognitive therapy takes effect.
Applications
Research has proven these drugs work. Antipsychotics have long been established as a relatively cheap, effective treatment, which quickly reduce symptoms and enable many people to live relatively normal lives (Van Putten, 1981). Relapse is likely when patients stop taking the drugs. Drug treatment is usually superior to no treatment at all. Between 50–65% of patients benefit from drug treatments.
One of the big positives of drug therapy is that it requires very little effort from the client; they just have to take some pills. However, this is not always true as most doctors use drug therapy alongside another treatment, like counseling or family therapy. This is an "integrated approach".
However, there's a risk that patients stop taking their medication. They may do this because they don't understand their illness, because their relationship with their clinician isn't very good or because they don't like the side-effects. Rosenhan (1973) instructed his pseudopatients to flush their medication down the toilet and they discovered that the other genuine patients were doing the same.
Research has proven these drugs work. Antipsychotics have long been established as a relatively cheap, effective treatment, which quickly reduce symptoms and enable many people to live relatively normal lives (Van Putten, 1981). Relapse is likely when patients stop taking the drugs. Drug treatment is usually superior to no treatment at all. Between 50–65% of patients benefit from drug treatments.
One of the big positives of drug therapy is that it requires very little effort from the client; they just have to take some pills. However, this is not always true as most doctors use drug therapy alongside another treatment, like counseling or family therapy. This is an "integrated approach".
However, there's a risk that patients stop taking their medication. They may do this because they don't understand their illness, because their relationship with their clinician isn't very good or because they don't like the side-effects. Rosenhan (1973) instructed his pseudopatients to flush their medication down the toilet and they discovered that the other genuine patients were doing the same.
Being medicated involves the admission of needing someone else’s help…It is an admission of some degree of helplessness - Jack Bergen
James Stone (2012) refers to the "new dawn" of antipsychotic medication: drugs that target glutamate rather than dopamine. These drugs are still in clinical trials but they promise to reduce positive and negative symptoms without the harmful side-effects of drugs that target dopamine. The theory behind this is reviewed in the contemporary study into schizophrenia by Carlsson et al. (1999).

|
EXEMPLAR ESSAY
|