
|
BIOLOGICAL TREATMENTS FOR DEPRESSION
The Unit 2 Exam expects you to know about one biological treatment for a disorder other than schizophrenia; this page considers unipolar depression. and drug therapy (also known as pharmacotherapy or chemotherapy).
You are also expected to understand a biological explanation of depression which is linked to this treatment. There are other biological treatments besides drug therapy. For example, there is shock therapy (electro-convulsive therapy or ECT) but this is uncommon (and unethical) in 21st century medicine.
|

|
PRESCRIBING ANTIDEPRESSANTS FOR UNIPOLAR DEPRESSION
|
|
These antidepressants had been discovered accidentally, but now that researchers understood how they worked, new antidepressants were developed to produce the same effects without the side-effects. These "third generation" drugs were developed in the 1980s and '90s and worked by preventing the reuptake of serotonin in particular, boosting the amount of serotonin active in the synapses but leaving other neurotransmitters like dopamine unaffected. These are known as selective serotonin reuptake inhibitors (SSRI). The most famous brand of SSRI is Prozac which became the most-prescribed antidepressant in America by the 1990s.
|
A one-and-a-half minute summary of SSRIs
|
SSRIs have fewer side-effects than the earlier antidepressants, but there are still adverse reactions, like headaches, weight gain, lethargy, nausea and sexual problems.
SSNI drugs followed, which prevent the reuptake of noradrenaline (norepinephrine) and leave the other neurotransmitters unaffected. SSNIs are also effective for people with anxiety disorders or obsessive compulsive disorder (OCD). They have similar side-effects to SSRIs.
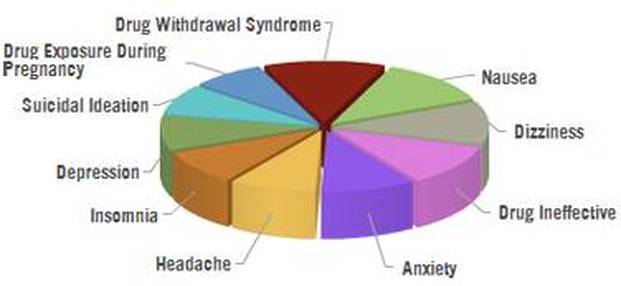
Top 10 side-effects of antidepressants. "Suicidal ideation" means compulsive thoughts about suicide. Notice that, for some people, depression is a side-effect of antidepressants, which is a cruel irony.
In this 5-minute video, Julie sums up the biological explanation and how antidepressants work - including neurogenesis and the importance of the hippocampus

|
APPLYING BIOLOGICAL TREATMENTS FOR DEPRESSION
|
|
Prozac Nation was a 1994 bestseller in which Elizabeth Wurtzel describes her battle with depression. It was made into a film in 2001 with Christina Ricci playing Wurtzel. It doesn't pull any punches - and Wurtzel is a less-than-likeable character - but Ricci is fantastic and it gives an insight into the experience of unipolar depression and life on antidepressants.
|
|
Crash Course Psychology looks at biomedical treatments - psychotropic drugs are at 5:00
|
EVALUATING BIOLOGICAL TREATMENTS
|
|
Some critics argue that antidepressants are a "placebo" - they only work because the patient believes they will work. This was tested by Kirsch et al (2008) who reviewed 47 trials of patients with mild or severe depression who were prescribed SSRI antidepressants or a placebo (sugar pill) that looked like an antidepressant. The patients with severe depression did show a statistically greater response to antidepressants than to placebos. This suggests that antidepressants do work - but that a lot of their effectiveness can be explained by the Placebo Effect because patients feel better if they believe in the treatment they are getting (even if it doesn't do anything).
|
|
Objections
Drug therapy doesn't work for everyone. Although more patients respond to the SSRIs than to the first generation antidepressants, this is still not all patients. It is estimated only 70% of patients benefit from drug treatments.
All the drugs used to treat depression have adverse reactions; these could include weight gain, nausea and drowsiness. Some people feel the side-effects are worse than the symptoms they are alleviating. The Recovery Model takes a different approach, urging people with depression to stop taking drugs and find different ways of living with their symptoms.
The Recovery Movement makes some good points but also advocates a lot of conspiracy theories, like the idea that the medical drugs companies ("Big Pharma") deliberately push medication onto people to boost their own profits.
Nonetheless, there is a growing concern that antidepressants are being over-prescribed. The study by Kirsch et al. (2008) caused a stir by showing that SSRIs weren't any better than placebos when it came to mild depression. This would mean doctors were prescribing pills that carried side-effects but weren't doing mildly depressed patients any good (and perhaps weren't doing severely depressed patients enough good to justify the side-effects).
Nonetheless, there is a growing concern that antidepressants are being over-prescribed. The study by Kirsch et al. (2008) caused a stir by showing that SSRIs weren't any better than placebos when it came to mild depression. This would mean doctors were prescribing pills that carried side-effects but weren't doing mildly depressed patients any good (and perhaps weren't doing severely depressed patients enough good to justify the side-effects).
while many people may benefit from antidepressant treatment (although most of them to a degree that is not clinically significant), about 1 in 4 are made worse - Irving Kirsch
|
Irving Kirsch is Associate Director at the Centre for Placebo Studies and his 2008 research project involved the University of Hull. In 2010, Kirsch published The Emperor's New Drugs: Exploding the Antidepressant Myth. In 2014, the British Psychological Society included Kirsch's placebo study in their "Ten Most Controversial Psychology Studies Ever Published".
|
|
In the UK, over 40 million antidepressants are prescribed every year and, in the United States, 1 person in 10 has been prescribed antidepressants and 1 in 6 of those taking antidepressants aren't depressed or sufffering from any mental disorder This is partly due to the huge popularity of Prozac, which acquired a reputation as a "happiness pill" that could improve the quality of life for people with normal moods as well as people with mood disorders.
This links to concerns about the medicalisation of normal experience - ordinary people are turning to powerful drugs to help them cope with life's ordinary ups and downs. |

|
|
|
Differences
The great advantage of CBT over drug therapy is the lack of side-effects. On the other hand, cognitive therapy can be more threatening for some patients, because you have to open up and talk about your problems. For some people, popping a pill is preferable to sharing unpleasant thoughts and feelings with a therapist.
Both treatments take time to be effective: drug therapy takes weeks, cognitive therapy takes months. This means a patient who is very distressed and perhaps suicidal will get much more help in the short term from antidepressants.
However, in the long term, CBT might be more beneficial. Treatments can either cure the disorder or suppress the symptoms without changing the underlying problem (palliative treatments). Drug therapy for unipolar depression is palliative rather than curative, which is why there are high relapse rates when the drugs are stopped. CBT is curative instead.
Hollon et al. (2005) studied patients who received treatment for 16 weeks then were observed for 12 months to see if their symptoms returned (relapse). There were 3 groups: (1) patients who received CBT; (2) patients who received drug therapy; and (3) patients received drug therapy which continued over the 12 month observation period. Only 31% of CBT patients suffered a relapse compared to 76% of those treated with drugs and 47% of the patients who carried on taking antidepressants. These findings show that drug therapy is only palliative whereas cognitive therapy offers a better cure.
The NHS recommends an "integrated approach" involves combining the two treatments. Antidepressants might give some patients the confidence and concentration to take part in CBT. It may be possible to reduce the dependency on antidepressants as the cognitive therapy takes effect.
Both treatments take time to be effective: drug therapy takes weeks, cognitive therapy takes months. This means a patient who is very distressed and perhaps suicidal will get much more help in the short term from antidepressants.
However, in the long term, CBT might be more beneficial. Treatments can either cure the disorder or suppress the symptoms without changing the underlying problem (palliative treatments). Drug therapy for unipolar depression is palliative rather than curative, which is why there are high relapse rates when the drugs are stopped. CBT is curative instead.
Hollon et al. (2005) studied patients who received treatment for 16 weeks then were observed for 12 months to see if their symptoms returned (relapse). There were 3 groups: (1) patients who received CBT; (2) patients who received drug therapy; and (3) patients received drug therapy which continued over the 12 month observation period. Only 31% of CBT patients suffered a relapse compared to 76% of those treated with drugs and 47% of the patients who carried on taking antidepressants. These findings show that drug therapy is only palliative whereas cognitive therapy offers a better cure.
The NHS recommends an "integrated approach" involves combining the two treatments. Antidepressants might give some patients the confidence and concentration to take part in CBT. It may be possible to reduce the dependency on antidepressants as the cognitive therapy takes effect.
Applications
Antidepressants have long been established as a relatively cheap, effective treatment, which quickly reduce symptoms and enable many people to live relatively normal lives. Relapse is likely when patients stop taking the drugs. Drug treatment is usually superior to no treatment at all. Around 70% of patients benefit from drug treatments.
One of the big positives of drug therapy is that it requires very little effort from the client; they just have to take some pills. However, this is not always true as most doctors use drug therapy alongside another treatment, like counseling or family therapy. This is an "integrated approach".
However, there's a risk that patients stop taking their medication. They may do this because they don't understand their illness, because their relationship with their clinician isn't very good or because they don't like the side-effects.
Researchers like Irving Kirsch argue that antidepressants are really placebos and do little good for all but the most severely depressed patients. If Kirsch is right, we should cut down the amount of antidepressants we prescribe and focus more on counseling and cognitive therapies.
One of the big positives of drug therapy is that it requires very little effort from the client; they just have to take some pills. However, this is not always true as most doctors use drug therapy alongside another treatment, like counseling or family therapy. This is an "integrated approach".
However, there's a risk that patients stop taking their medication. They may do this because they don't understand their illness, because their relationship with their clinician isn't very good or because they don't like the side-effects.
Researchers like Irving Kirsch argue that antidepressants are really placebos and do little good for all but the most severely depressed patients. If Kirsch is right, we should cut down the amount of antidepressants we prescribe and focus more on counseling and cognitive therapies.
|
EXEMPLAR ESSAY
|