

|
The Specification says you need to know about "effect of recreational drugs on the transmission process in the central nervous system" - but it doesn't specify which drugs in particular. I'm offering two examples: nicotine and amphetamines (cocaine) because they have different effects: one is a dopamine agonist and the other a reuptake antagonist.
|
|
THE NEUROBIOLOGY OF RECREATIONAL DRUGS
Drugs are chemicals that have an effect on humans. Recreational drugs alter humans' thought processes (cognitions), mood and behaviour. These changes are usually enjoyable in some way, even though the after-effects may not be. Recreational drugs are also termed "drugs of abuse" because of the long-term dangers they produce. They are sometimes called psychoactive drugs because they have an effect on the central nervous system (CNS).
|
|
Reward Pathways & Pleasure Centres
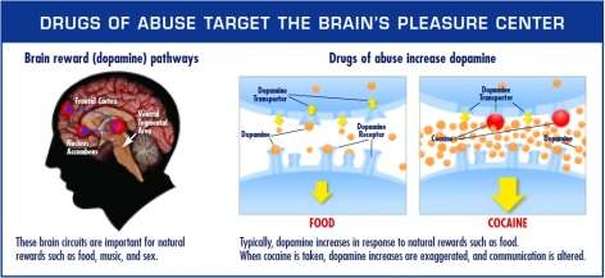
Recreational drugs are pleasurable because the affect the reward pathway in the brain. This isn't a literal "path" but it is a route through the brain used by a neurotransmitter called DOPAMINE.
DOPAMINE is a neurotransmitter associate with REWARD. It creates feelings of pleasure and a desire to repeat whatever activity you are doing when the dopamine flows. Dopamine is generated naturally in the brain when we do activities like eating or drinking. Some neurons are DOPAMINERGIC - they generate dopamine and respond to dopamine. A "pathway" of these dopaminergic neurons is a PLEASURE CENTRE. One of these dopaminergic pathways is the mesolimbic pathway that flows through the limbic system of the brain where our basic desires and appetites are located.
Dopamine normally produces sensations of satisfaction and contentment, but a rush of dopamine can produce a more intense sensation of EUPHORIA (pleasure). This can happen naturally (for example, during sex, or when drinking a glass of cool water when you're very thirsty), but recreational drugs trigger euphoria artificialy. Recreational drugs tend to work in two different ways:
|


|
APPLYING THE NEUROBIOLOGY OF DRUGS TO REAL LIFE
|
|
Nicotine
Nicotine is the psychoactive chemical in cigarettes. Nicotine mimics a natural neurotransmitter called ACETYCHOLINE. Nicotine enters the blood when it is inhaled (or through a gum or patch) and when it arrives in the brain it attaches acetycholine receptors - also called nicotine receptors. The receptors excite the neuron, causing it to release dopamine, which in turns excites the neighbouring neurons in the reward pathway. This produces feelings of pleasure. This slightly pompous video gives more detailed terminology. Notice a useful piece of vocabulary: nicotine is an acetycholine AGONIST - an agonist is a chemical that excites receptors.
It's important to remember that the brain is PLASTIC - it changes its structure in response to what we do. If nicotine receptors are over-used, the brain responds by cutting back on the nearby dopamine receptors. This means more dopamine is needed to produce a nornal level of functioning. This explains DESENSITISATION: at first, nicotine has a big effect but over time larger and larger doses of nicotine are needed to get the pleasurable sensation. It also explains ADDICTION, because, without nicotine, the brain is not generating enough dopamine, so the user feels unhappy until they have their next smoke.
There are of course other explanations of addiction - such as the Learning Approach.
Several other drugs work in a similar way to nicotine: opiates (like heroin) bond to opioid receptors and cannabis bonds to cannabinoid receptors.
Amphetamines (Cocaine)
Amphetamines work differently, although they still affect dopamine reward pathways. In a normal brain, dopamine is re-absorbed back into the neurons. This process is called RE-UPTAKE. Amphetamines block this process. For example, cocaine attaches to the reuptake receptor, 'blocking' it so that dopamine cannot be re-absorbed back into the neuron. This means the levels of dopamine in the synaptic gap (the space between neurons) keeps building and building. The dopamine receptors get over-stimulated. This isn't a foreign substance binding to the dopamine receptors - it's 'natural' dopamine in massive quantities. A short plain-language BBC video (it refers to dopamine as a "feel-good neurotransmitter", which it is, but you should avoid such expressions in the exam).
Brain PLASTICITY means that long term use of amphetamines has a similar result to long term use of nicotine. The number of dopamine receptors decreases in response to the excess of dopamine. This means larger doses of cocaine are needed to recapture the original pleasure (desensitisation) and that, without cocaine in the system, the brain's reward pathways don't work properly, leading to unhappiness and cravings (addiction).
Hank from Crash Course describes the neurobiology of drugs and links it to other addictions, like gambling
|
|
EVALUATING THE NEUROBIOLOGY OF DRUGS
|
|
The rats could give their brains a pleasurable electric shock by pressing a lever. Olds & Milner noticed that the rats would return to the lever over and over, ignoring other sources of pleasure like food or rats of the opposite sex. In other words, they behaved rather like drug addicts.
The existence of pleasure centres links to Skinner's theory of Operant Conditioning. |
Olds & Milner's study is described at 2.00 minutes
|
Studies like Olds & Milner are carried out on animals in lab conditions. They are easily replicated. For example, Straiker & Mackie (2005) carried out a similar study on mice; genetic technology was used to give the mice cannibinoid receptors and the mice showed similar addictive behaviour to humans when dosed with cannabis.
There's also face validity to this explanation: observations of drug-users and self-reports from drug-users tend to match what the neurobiology of recreational drugs would predict. For example, the sensation of euphoria when the drug is taken and the experiences of desensitisation and addiction with long-term use.
However, not all recreational drugs work on dopamine. For example, PCP ("angel dust") and ketamine produce intense euphoria, but instead of activating dopamine they stimulate glutamate receptors called NMDA.
There's also face validity to this explanation: observations of drug-users and self-reports from drug-users tend to match what the neurobiology of recreational drugs would predict. For example, the sensation of euphoria when the drug is taken and the experiences of desensitisation and addiction with long-term use.
However, not all recreational drugs work on dopamine. For example, PCP ("angel dust") and ketamine produce intense euphoria, but instead of activating dopamine they stimulate glutamate receptors called NMDA.
Objections
Generalising from animal studies to humans is problematic. Humans have much more complex cognitions than animals: they use drugs for reasons. For example, they use recreational drugs to regulate their mood, cope with stress, bond socially with friends or even out of curiosity or as a lifestyle statement. Neurobiological explanations ignore all these choices and motivations, treating drug users as slaves to their own neurobiology, helplessly chasing the drug-induced euphoria. In other words, this sort of explanation is REDUCTIONIST.
Generalising from animal studies to humans is problematic. Humans have much more complex cognitions than animals: they use drugs for reasons. For example, they use recreational drugs to regulate their mood, cope with stress, bond socially with friends or even out of curiosity or as a lifestyle statement. Neurobiological explanations ignore all these choices and motivations, treating drug users as slaves to their own neurobiology, helplessly chasing the drug-induced euphoria. In other words, this sort of explanation is REDUCTIONIST.
There is also the problem of the PLACEBO EFFECT. This is when people experience psychological and biological changes because they believe a drug will affect them rather than because of any chemical agent involved. Jones & Stone (1990) gave regular cannabis users either marijuana (which contains cannabis) or a placebo (which seemed to be marijuana but contained no cannabis). The users could not detect the difference.
If the effects of drugs were entirely biological, the placebo group should have experienced no effect. The fact that they experienced a "high" just like the marijuana group suggests there is a cognitive element to drug-taking as well as a biological element.
If the effects of drugs were entirely biological, the placebo group should have experienced no effect. The fact that they experienced a "high" just like the marijuana group suggests there is a cognitive element to drug-taking as well as a biological element.
Differences
There are SIMILARITIES between the neurobiological view of recreational drugs and the Learning Approach:
- Both involve the idea of euphoria/pleasure as the main reason people take drugs and keep taking them. In Operant Conditioning, this is called POSITIVE REINFORCEMENT
- Both explain addiction through the unpleasant side-effects of not taking the drug. In Operant Conditioning, this is NEGATIVE REINFORCEMENT.
- Research like Olds & Milner (1954) backs up Skinner's research into operant conditioning in rats and pigeons.
|
Freud's psychodynamic approach would look at drug use differently. Freud would focus on the MEANING the drug use had for the user; in particular, he would focus on childhood traumas or family conflicts that were behind the drug use.
|
Freud, holding one of his recreational drugs
|
Freud agrees with the other approaches that PLEASURE is the root cause of drug-taking. However, he thinks that SEXUAL PLEASURE (eros) is the main motivation and drugs are a substitute for a sexual pleasure that the user cannot achieve or which the user finds upsetting. In other words, drug taking is a DEFENCE MECHANISM. It might help the user REPRESS unwanted sexual impulses or it might be a DISPLACEMENT of a sexual urge.
|
Freud himself was an early defender of cocaine as a cure for psychological problems. In fact, Freud's reputation has been rather damaged by his enthusiasm for cocaine and his use of it on his patients.
More generally, Freud's concepts (like defence mechanisms) are not empirically (scientifically) observable, making them impossible to prove or disprove. |
|
Applications
The neurobiological explanation of drugs has led to biological treatments for addiction.
Drug Replacement Therapy (DRT) involves giving the user a substitute for the drug that produces a similar euphoria but in a controlled way. Gradually the dosage is cut back. This deals with the problems of desensitisation and addiction because, once the user is taking only very small amounts of the drug, the brain's dopamine receptors will return to a normal level of functioning. The user can then quit.
Drug Replacement Therapy (DRT) involves giving the user a substitute for the drug that produces a similar euphoria but in a controlled way. Gradually the dosage is cut back. This deals with the problems of desensitisation and addiction because, once the user is taking only very small amounts of the drug, the brain's dopamine receptors will return to a normal level of functioning. The user can then quit.
Examples of DRT include:
- Methadone is a substitute for heroin
- Nicotine patches and nicotine gum are substitutes for cigarettes
DRT only tackles the neurobiology of drug addiction; if the user doesn't want to quit then they won't take the final step. This is why they work best when combined with some sort of cognitive therapy that gets the user to re-think their priorities and choices.
Davidson et al. (1998) tested the effectiveness of nicotine patches compared to a placebo group whose patches didn't contain any nicotine. After 6 weeks, 20% of the DRT group had quit smoking compared to 8% of the placebo group. This suggests that DRT is more effective than willpower alone.
Davidson et al. (1998) tested the effectiveness of nicotine patches compared to a placebo group whose patches didn't contain any nicotine. After 6 weeks, 20% of the DRT group had quit smoking compared to 8% of the placebo group. This suggests that DRT is more effective than willpower alone.
The main application of Freud's theories is the therapy called psychoanalysis.
Psychoanalysis can help treat aggression by exploring the unconscious causes of addiction. The psychoanalyst helps the client explore their own dreams and childhood memories and work out what they mean. Hopefully, the client will learn about the defence mechanisms they are using and the unresolved conflicts going on in their unconscious. They may come to self-knowledge.
Psychoanalysis can help treat aggression by exploring the unconscious causes of addiction. The psychoanalyst helps the client explore their own dreams and childhood memories and work out what they mean. Hopefully, the client will learn about the defence mechanisms they are using and the unresolved conflicts going on in their unconscious. They may come to self-knowledge.
The main criticism of psychoanalysis as a cure for addiction is that it is time-consuming, expensive and not at all certain to work. Since it is not scientifically-based, it is difficult to measure how effective it is and whether or not it is working for any particular client.

This is AO1 - describing the biological view
This is AO2 - arguing for the credibility of the explanation, using research in support then criticising the explanation
More AO1, describing the explanation in more detail
Back to AO3 - arguing that the explanation has good applications
The conclusion offers more AO3, arguing for a balanced view |
EXEMPLAR ESSAY
|