
|
This mental disorder is compulsory so every candidate learns it and the Examiner will expect you to know it in detail. The Specification identifies HALLUCINATIONS, DELUSIONS, THOUGHT INSERTION and DISORDERED THOUGHTS in particular, so you could be asked about these. Make sure you understand the difference between the FEATURES of schizophrenia (how common it is, what sort of people develop it?) and the SYMPTOMS (what thoughts or behaviours do people with the disorder show?).
|
|
SCHIZOPHRENIA
In Unit 2, Clinical Psychology expects all students to know about schizophrenia, its features and symptoms as well as different explanations and treatments.
People with schizophrenia often have an altered perception of reality. They may see or hear things that don’t exist, speak in strange ways, believe that others are trying to harm them or feel like they’re being constantly watched (paranoia). This can make daily life difficult, so people with schizophrenia may withdraw from the outside world or act out in confusion. Schizophrenia is a chronic disorder, meaning that once you have it, it does not go away. However, with support, medication and therapy, many people with schizophrenia can function independently and live fulfilling lives.
| ||||||

|
FEATURES OF SCHIZOPHRENIA
|
|
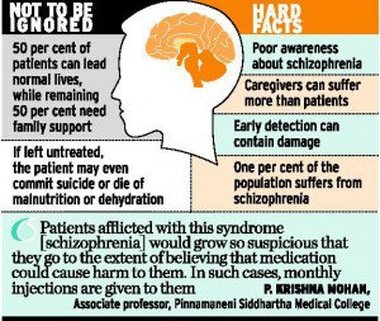
Schizophrenia is one of the more common mental disorders. 1% of the population will be affected by it in their life. Symptoms usually appear in early adulthood. It affects men and women equally, but the symptoms usually appear earlier in men (teens) and later in women (20s or 30s).
A quarter of people with schizophrenia suffer one episode but then recover; another quarter do not recover and have the symptoms for the rest of their lives. Half of people with schizophrenia can, with treatment, go through periods without symptoms but the symptoms recur. |
|
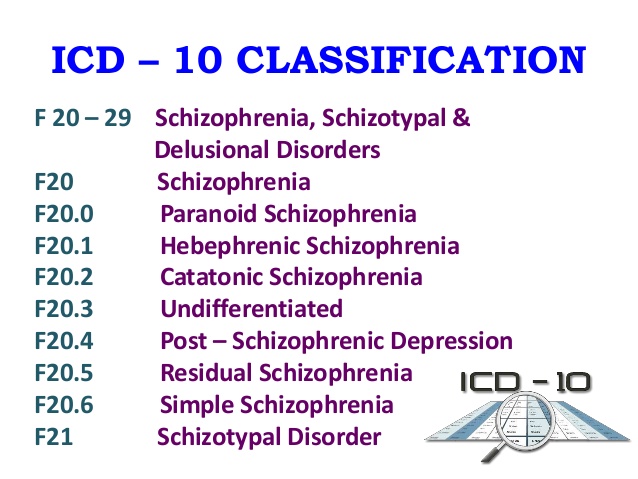
ICD-10 codes schizophrenia as F20 and lists 7 types of schizophrenia.
Paranoid schizophrenia (F20.0) is the most common type, tending to develop later and having more positive symptoms. Hebephrenic (or disorganised) schizophrenia (F20.1) develops earlier and involves confused emotions. Catatonic schizophrenia (F20.2) is very rare and sufferers are motionless and silent. Undifferentiated (F20.4) is a mixture of symptoms of the other types. Simple schizophrenia (F20.6) is rare and features only negative symptoms. |
|
DSM used to include similar types of schizophrenia but DSM-5 has replaced them with a single category: schizophrenia spectrum disorders. This is because schizophrenia features a range (spectrum) of symptoms which are not fixed but might change over time.
FAMOUS PEOPLE WITH SCHIZOPHRENIA
Brian Wilson - founded the Beach Boys, wrote Good Vibrations
|

John Nash - Nobel Prize-winning mathematician, subject of A Beautiful Mind (2001)
|

Vivien Leigh - Oscar-winning actress, played Scarlet O'Hara in Gone With The Wind (1939)
|

Vincent Van Gogh - Dutch artist, painted Sunflowers, appeared in Doctor Who
|

Jake Lloyd - actor, played Young Anakin Skywalker in The Phantom Menace (1999)
|

Joey Ramone - punk rock icon, lead singer in The Ramones
|
|
The 2001 film A Beautiful Mind stars Russell Crowe as John Nash. It plays tricks with the audience and takes liberties with history, but it gives some insight into the positive symptoms of schizophrenia and the problems with therapy - as well as being a great film.
The idea of schizophrenia as a 'beautiful' condition is also suggested in Don McLean's Vincent - a song tribute to Vincent Van Gogh. |
|

|
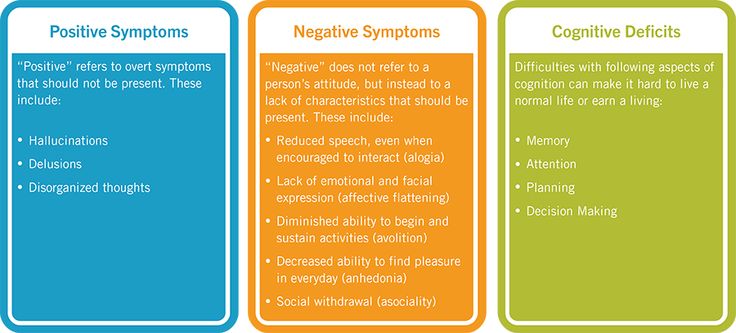
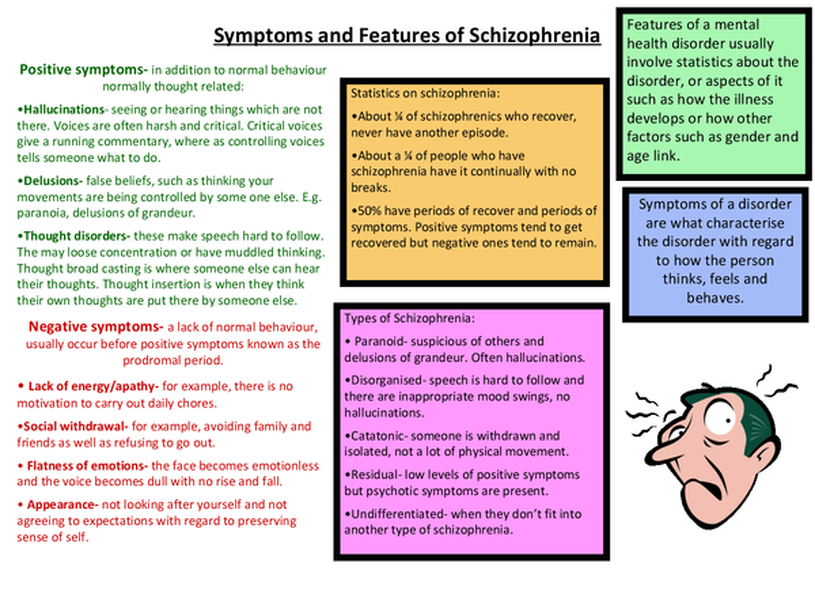
SYMPTOMS OF SCHIZOPHRENIA
|
|
EVALUATING THE DIAGNOSIS OF SCHIZOPHRENIA
|