
|
DEPRESSION
In Unit 2, Clinical Psychology expects all students to know about one disorder from this list: anorexia nervosa, obsessive-compulsive disorder (OCD) and unipolar depression. In addition to the features and symptoms, you will need to study:
Unipolar depression (or clinical depression or just 'depression') is a mood disorder. It is different from schizophrenia because it is non-psychotic. The depressed person understands the difference between imagination and reality and recognises that their own depressed mood may be irrational or inappropriate, but can't help feeling the way they do.
Be careful not to confuse depression with bipolar disorder (sometimes called manic-depression), in which a person goes from periods of depressed mood to periods of 'manic' energy and restlessness.
5-minute video with a particular focus on symptoms and biological explanations
| ||||
|
FEATURES OF UNIPOLAR DEPRESSION
|

Robin Williams - actor & comedian, committed suicide in 2016
|

Oprah Winfrey - actress and TV presenter
|

Caroline Aherne - actress & writer, died in 2016
|

Sylvia Plath - writer & poet
|

Stephen Fry - actor, writer & presenter
|

Winston Churchill - prime minister & war leader
|
|
|
British Prime Minister a war leader Winston Churchill suffered from depression. He referred to his condition as a "black dog" that followed him. He frequently thought about suicide. During severe bouts of depression he couldn't function at all and, at other times, drank heavily to conceal the symptoms. His doctor prescribed him amphetamines.
|
|
The 1999 film The Virgin Suicides was directed by Sofia Coppola and deals with depression. It tells the story of the Lisbon sisters from the perspective of the neighborhood boys who are in love with them. The girls' mental health issues lead to a tragic conclusion.
If you don't like the film, you'll still love the sublime soundtrack by the French band Air. |
|

|
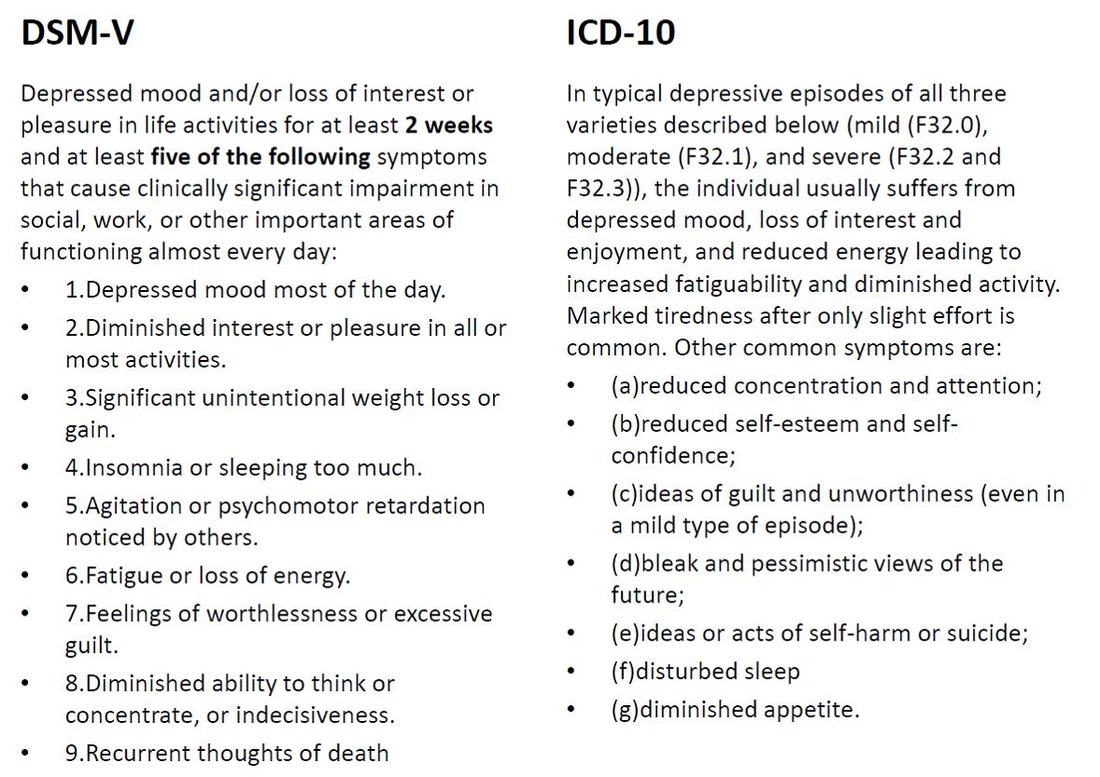
SYMPTOMS OF UNIPOLAR DEPRESSION
|
|
EVALUATING THE DIAGNOSIS OF DEPRESSION
|