

|
DEVELOPMENT, GENES & THE BRAIN
Development describes how a creature changes over time. It include changes brought about by the environment (nurture) but we will be looking in more detail at changes brought about through maturation (nurture).
Maturation includes all the changes that occur for biological reasons. These can be broken into several stages of development:
We now understand that maturation is shape by genes.
A gene is a set of biological information contained on a strand of DNA. At conception, each human acquires 50% of their genes from each parent. Genes are inherited. The complete description of all your genes is your genotype. What you actually turn into and how your behave when all your genes interact with each other and with your environment is your phenotype. Even people with the same genotype (such as identical twins) may have different phenotypes.
|
|
THE ROLE OF GENES IN DEVELOPMENT
|

|
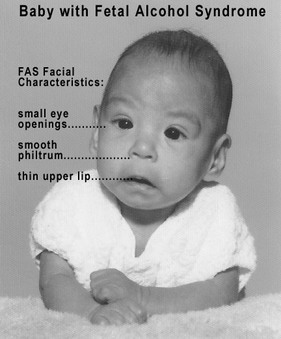
Drinking excessive alcohol while pregnant can cause foetal alcohol spectrum (FAS). It is unknown how much alcohol is needed to cause damage, and so many doctors recommend completely avoiding alcohol during pregnancy. Children with FAS may have a small head size and abnormal facial features. They also tend to have poor impulse control, learning difficulties and lower IQ scores. These problems carry on into adulthood (Streissguth et al., 2004).
You may have noticed "poor impulse control" and made a connection to Eysenck's psychoticism (P) trait. You did? Good!
|
|
POST-NATAL DEVELOPMENT
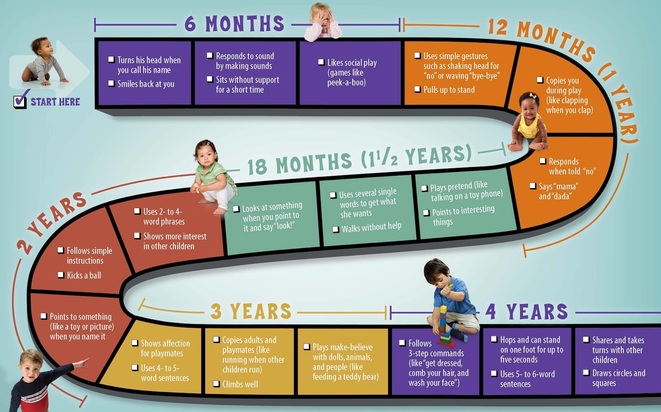
After they are born, infants develop motor skills (movement). Gross motor skills involve groups of muscles to do things like stand up, walk and jump. Most children can do these things by the end of their second year. As they mature (4-5 years), they develop more complicated gross motor skills, like riding bikes or catching balls.
Fine motor skills are more precise, use fewer muscles but often involve hand-eye coordination. This includes eating with spoons and forks, drawing, using buttons and tying laces.
Fine motor skills are more precise, use fewer muscles but often involve hand-eye coordination. This includes eating with spoons and forks, drawing, using buttons and tying laces.
Again, you don't need to know most of this, but it's helpful to be able to give one example of children's maturation at a certain age.
Brain development happens very quickly. The brain grows faster than any other organ in a child's body. Neurons forms and synapses develop between them. At birth, a child's brain is only 30% of its adult weight; by age 2 it is 70% of its adult weight.
This is accompanied by emotional development. Children develop emotional self-regulation: the ability to understand and control their own emotions. It involves restraining some emotional responses or delaying them so that they can be shown in a more appropriate way later. The classic example is holding your temper.
This is accompanied by emotional development. Children develop emotional self-regulation: the ability to understand and control their own emotions. It involves restraining some emotional responses or delaying them so that they can be shown in a more appropriate way later. The classic example is holding your temper.
Eysenck's neuroticism (N) trait reflects how difficult someone finds emotional self-regulation; very difficult for high-N individuals
There is also a development of empathy, the ability to recognise and understand other people's emotions. Children who possess empathy are less likely to be antisocial.
Eysenck's psychoticism (P) trait reflects how difficult someone finds empathy; very difficult for high-P individuals
ADOLESCENT DEVELOPMENT
Adolescence begins at puberty and ends with adulthood and usually covers the 10-18 age range.
Hormones drive physical changes in adolescence, but the release of hormones is dictated by genes. In addition, environmental factors like diet and exercise also influence the release of hormones (for example, puberty begins earlier if you are overweight). The release of hormones in adolescence is controlled by the pituitary gland.
Testosterone is the male growth hormone; oestrogen is the female growth hormone. During adolescence, growth hormones increase height, muscle mass and lead to the growth of secondary sexual characteristics (breasts, body hair). There is a redistribution of body fat and an increase in the size of lung and heart, leading to more strength and stamina.
Hormones drive physical changes in adolescence, but the release of hormones is dictated by genes. In addition, environmental factors like diet and exercise also influence the release of hormones (for example, puberty begins earlier if you are overweight). The release of hormones in adolescence is controlled by the pituitary gland.
Testosterone is the male growth hormone; oestrogen is the female growth hormone. During adolescence, growth hormones increase height, muscle mass and lead to the growth of secondary sexual characteristics (breasts, body hair). There is a redistribution of body fat and an increase in the size of lung and heart, leading to more strength and stamina.
|
The brain develops in this period and there are big changes in the frontal lobes, which continue to mature right up until the end of adolescence (Casey et al. 2005). Immature functioning of the frontal lobes might be responsible for risk-taking behaviour in adolescence. There are also changes in levels of serotonin and dopamine, especially in the limbic system, which increases emotionality.
|
Don't teach "Expelliarmus!" to someone whose frontal lobes are still maturing!
|
Eysenck's extroversion (E) and psychoticism (P) traits reflect a tendency towards risk-taking for high-P, high-E individuals; neuroticism (high-N) is linked to emotionality.
The adolescent brain works much faster than a child's brain, with processing speed peaking around age 15. There are improvements in attention, memory (especially working memory) and metacognition (which includes skills like planning ahead and interpreting things in different ways).
This new style of thinking is hard to get used to and adolescents may experience unusual thinking problems. The imaginary audience is a tendency for adolescents to imagine everyone is listing to them; the personal fable is a tendency to imagine that there will be no harmful consequences.
However, environmental changes are also going on. Adolescents distance themselves from their parents and develop new social relationships with peers. Cultural pressures begin to affect adolescents. These are pressures to conform to norms of behaviour regarding sex, belief, appearance and recreation. Adolescents can find it stressful to handle these new peer groups and cultural pressures. This makes it hard to tell whether development during adolescence is due to maturation or environmental factors.
This new style of thinking is hard to get used to and adolescents may experience unusual thinking problems. The imaginary audience is a tendency for adolescents to imagine everyone is listing to them; the personal fable is a tendency to imagine that there will be no harmful consequences.
However, environmental changes are also going on. Adolescents distance themselves from their parents and develop new social relationships with peers. Cultural pressures begin to affect adolescents. These are pressures to conform to norms of behaviour regarding sex, belief, appearance and recreation. Adolescents can find it stressful to handle these new peer groups and cultural pressures. This makes it hard to tell whether development during adolescence is due to maturation or environmental factors.
One example of biological/behavioural change during adolescence is all you will need.
ADULT DEVELOPMENT
Adults experience primary aging, which is normal maturation, but also biological changes due to lack of physical exercise and poor diet, which is secondary aging.
In early adulthood (ages 20–40), our physical abilities are at their peak, including strength, perception and heart functioning. Aging speeds up during middle adulthood (ages 40–65) with decline in vision, hearing, and immune-system functioning, as well as the end of reproductive capability for women (menopause). Hormonal changes take place during menopause, which may result in emotional swings, problems with attention and memory and changes in sexual interest.
During late adulthood (age 66+), reaction time slows further, muscle strength and mobility decrease, hearing and vision decline, and the immune system weakens.Many of the changes in the bodies and minds of older adults are due to a reduction in the size of the brain and loss of brain plasticity. Memory declines in old age. In general, an older person's procedural memory tends to remain stable, while working memory declines. In some cases, these changes mask the symptoms of dementia, including diseases like Alzheimer's.
In early adulthood (ages 20–40), our physical abilities are at their peak, including strength, perception and heart functioning. Aging speeds up during middle adulthood (ages 40–65) with decline in vision, hearing, and immune-system functioning, as well as the end of reproductive capability for women (menopause). Hormonal changes take place during menopause, which may result in emotional swings, problems with attention and memory and changes in sexual interest.
During late adulthood (age 66+), reaction time slows further, muscle strength and mobility decrease, hearing and vision decline, and the immune system weakens.Many of the changes in the bodies and minds of older adults are due to a reduction in the size of the brain and loss of brain plasticity. Memory declines in old age. In general, an older person's procedural memory tends to remain stable, while working memory declines. In some cases, these changes mask the symptoms of dementia, including diseases like Alzheimer's.
As with the previous sections, you only need to know one example of biological/behavioural changes in adulthood.
Your Key Question for the Cognitive Approach asks how psychology can help older people suffering from dementia.
Your Key Question for the Cognitive Approach asks how psychology can help older people suffering from dementia.
|
HUMAN DEVELOPMENT & EVOLUTION
|
|
You can see this at work in recessive genes like the genes for eye colour. These originally appeared as random mutations. In fact, the gene for blue eyes is called OCA2 and it first appeared in one human living over 6,000 years ago (Eiberg et al., 2008). The gene is neither positive nor negative for survival in itself, but when both the mother and the father carry the gene, there is a chance the child will receive OCA2 on both chromosomes and grow up to be blue-eyed.
|
Other genes have a more obvious survival value. In human beings, having a large brain has survival value. This is why we have inherited genes that programme our bodies to grow such large brains in our early years. This comes at a cost.
|
Many wild animals can stand up and walk within hours of being born. Human babies must usually be a year old before they can even begin to do this. This shows out is is a survival trait for animals to develop gross motor skills quickly. Human babies are working on their large brains and rely on their parents to protect them from dangers and bring them food. To help with this, we have evolved to become attached to our children and they become attached to us.
|
|
|
|
You can see the same evolutionary pressures at work during adolescence. With many animals, like cats, the young begin moving away from the mother and exploring their environment at a very young age. You can see young kittens practising hunting and fighting. It's cute! But human children stay under their parents' care until adolescence. Adolescence is when they start practising adult skills and behaviours. This is also because of the great amount of time it takes to grow a complete human brain.
|

|
APPLYING HUMAN DEVELOPMENT TO REAL LIFE
|

|
EVALUATING BIOLOGICAL DEVELOPMENT
|

|
EXEMPLAR ESSAY
|