
|
DIAGNOSING MENTAL DISORDERS
Diagnosis is proposing a cause for a medical problem (such as an infection or an injury). It is followed by prognosis, which is a prediction about how the problem will develop with or without treatment.
Diagnosing medical disorders takes place as part of a clinical interview, in which the therapist asks open-ended questions and the client describes their symptoms. The therapist will also make some observations (noticing you have a rash or that you have lost weight) and might use of biometric tools (like taking your temperature or giving you an X-ray). With mental disorders, diagnosis becomes more complicated. Often, the client cannot describe their symptoms very well and the therapist cannot make simple observations. There are no biometric tools for mental disorders. This is the old wisdom that, if someone says they have chest pains, you can measure their heart rate, but if someone says their heart is broken, there's no point in studying their heart. Mental disorders are often described poetically ("I feel very down!", "My life is over!") and although some brain scans correlate with mental disorders, that's not the same as showing the disorder itself.
Before diagnosing a mental disorder, we need to assess that it in fact is a disorder.
Assessments of abnormality are not based on any one criterion. Several different factors are considered. The main method of assessment used by clinical psychologists is the four Ds. |
|
The banner on this page is a reference to one of my favourite films, "Blade Runner", which is set in a future world where the police have to assess who is an android 'replicant' and who is really human. The opening scene features the bizarre "Voight-Kampff Test" which can tell the difference between humans and replicants.
It also has a great soundtrack by Vangelis! |
|

|
THE 4 Ds
|
|
The four Ds are used as an assessment tool to decide whether behaviour is abnormal. Abnormality may require investigation and diagnosis.
There is no clear difference between normal and abnormal - it's "shades of grey". This means that identifying a mental disorder using the four Ds is based on the therapist's judgement. When using the four Ds, a person's context and situation must be taken into account. Just because the four Ds are present, it doesn't automatically mean that person must be given a psychiatric diagnosis. |
Think about it: a lot of people who have strange jobs, unusual beliefs or extreme hobbies would fall under the 4 Ds, but they're still "normal".
|
DEVIANCE
These are behaviours and emotions that are viewed as unacceptable.
This leads to a question of whether deviance should be measured statistically (in terms of its rareness) or socially/culturally (in terms of social norms).
This leads to a question of whether deviance should be measured statistically (in terms of its rareness) or socially/culturally (in terms of social norms).
Statistical Definition of Deviance
One way of deciding whether behaviour is deviant is to consider how unusual it is. Behaviour is seen as normal if it occurs frequently but behaviour that occurs relatively rarely in the population is abnormal. Extremely rare people can be considered deviant.
Some behaviours can be measured on a quantitative scale; for example how extraversion levels can be measured by psychometric tests. At one end of the scale, there are the extreme extraverts who crave thrills and attention; at the other end of the scale are the introverts who are painfully shy.
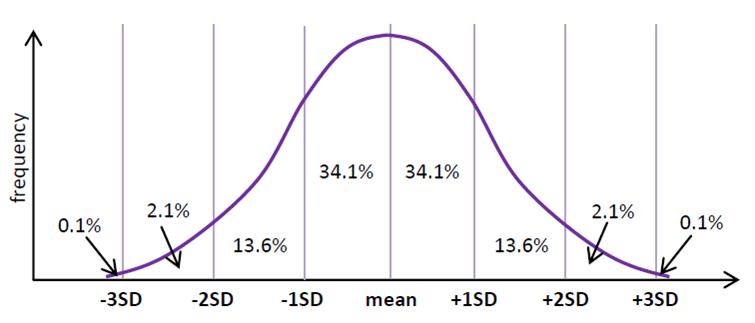
On a normal distribution curve, the majority of scores for a population will cluster around the mean. Any behaviour within the middle 68% of the population is seen as normal.
One way of deciding whether behaviour is deviant is to consider how unusual it is. Behaviour is seen as normal if it occurs frequently but behaviour that occurs relatively rarely in the population is abnormal. Extremely rare people can be considered deviant.
Some behaviours can be measured on a quantitative scale; for example how extraversion levels can be measured by psychometric tests. At one end of the scale, there are the extreme extraverts who crave thrills and attention; at the other end of the scale are the introverts who are painfully shy.
On a normal distribution curve, the majority of scores for a population will cluster around the mean. Any behaviour within the middle 68% of the population is seen as normal.
Standard deviation around the mean
This uses the idea of statistical deviation (SD). Normal people are within 1SD of the mean, falling within the 34.1% on either side in terms of their IQ, income, height, weight, age, level of extraversion, etc. "Odd" people are further from the mean - 2SD means in the 13.6% on either side of the normal people, so unusually clever or stupid, rich or poor, big or small, outgoing or shy. Truly abnormal people are in the 2.1% at the top or bottom of the scale: geniuses or dimwits, billionaires or beggars, giants or dwarfs, party animals or super-nerds.
This has the great advantage of defining abnormality (and therefore deviance) in objective, mathematical terms. The problem is, it ignores how we feel about abnormality. Some things are very rare, but quite harmless and even rather precious. Other things are quite common but we still disapprove of them.
Moreover, some mental disorders are actually quite common and getting more frequent. According to Wittchen et al. (2011), every year 165 million Europeans - 38.2% of Europe's population - suffer some form of mental illness, with the top 3 being anxiety, insomnia and depression.
This has the great advantage of defining abnormality (and therefore deviance) in objective, mathematical terms. The problem is, it ignores how we feel about abnormality. Some things are very rare, but quite harmless and even rather precious. Other things are quite common but we still disapprove of them.
Moreover, some mental disorders are actually quite common and getting more frequent. According to Wittchen et al. (2011), every year 165 million Europeans - 38.2% of Europe's population - suffer some form of mental illness, with the top 3 being anxiety, insomnia and depression.
Social Norms Definition of Deviance
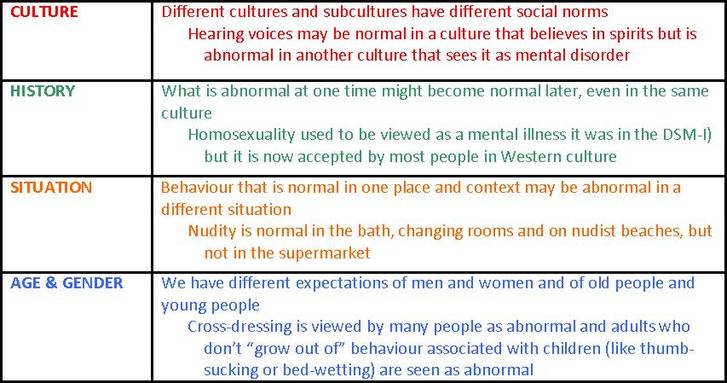
A social norm is an unwritten rule about acceptable behaviour. Norms are therefore the behaviours and attitudes that most people stick to in society. Norms can differ from culture to culture, and from time period to time period.
When people violate social norms, this is seen as abnormal. Most abnormal behaviour is harmless and abnormal people are treated as eccentric, or rebellious, rather than deviant. However, extremely abnormal behaviour conflicts with the values shared by the whole of society; people feel anxious or threatened by the person who is deviant.
There are a number of factors to take into account when assessing deviance based on social norms:
A social norm is an unwritten rule about acceptable behaviour. Norms are therefore the behaviours and attitudes that most people stick to in society. Norms can differ from culture to culture, and from time period to time period.
When people violate social norms, this is seen as abnormal. Most abnormal behaviour is harmless and abnormal people are treated as eccentric, or rebellious, rather than deviant. However, extremely abnormal behaviour conflicts with the values shared by the whole of society; people feel anxious or threatened by the person who is deviant.
There are a number of factors to take into account when assessing deviance based on social norms:
This has the great advantage of defining abnormality (and therefore deviance) in terms of popular feelings and moral values - it is behaviour that frightens or outrages other people. However, it's a rather subjective assessment. There's a risk that the therapist will be influenced by whether they personally find behaviour shocking or upsetting, rather than be what society-at-large feels. It can be difficult to find out what social norms in general are. On many topics, society is quite divided about what should be viewed as normal.
DYSFUNCTION
This is when the abnormal behaviour is significantly interfering with everyday tasks and living your life.
Under this definition, a person is considered abnormal if they are unable to cope with the demands of everyday life - looking after yourself, holding down a job, maintaining relationships with friends and family, making yourself understood etc.
Rosenhan & Seligman (1989) suggest the characteristics that define failure to function adequately:
Dysfunction gets across the idea of a behaviour getting in the way of living a healthy life (which the statistical definition of deviance ignores) but it's a bit more objective than appealing to social norms. For example, even if a person's sexuality is unusual or shocking to other people, if they can still lead a healthy life then they're not abnormal.
A problem with this is that abnormal behavior may actually be helpful for the individual. For example, taking drugs might help people with stressful jobs or help artists unlock their creativity. In fact, there might be some social groups where not taking drugs is dysfunctional behaviour.
Under this definition, a person is considered abnormal if they are unable to cope with the demands of everyday life - looking after yourself, holding down a job, maintaining relationships with friends and family, making yourself understood etc.
Rosenhan & Seligman (1989) suggest the characteristics that define failure to function adequately:
- Unpredictably & loss of control (no one knows what you'll do next, not even you)
- Irrationality/incomprehensibility (no one understands you, you don't even understand yourself)
- Cause discomfort to observers (you upset, frighten or annoy everyone with your behaviour)
- Suffering (the same as distress, below)
- Maladaptiveness (you are a risk to yourself and others; see danger below)
- Vividness & unconventionality (you stand out; see deviance above)
- Violate moral standards (similar to deviance)
Dysfunction gets across the idea of a behaviour getting in the way of living a healthy life (which the statistical definition of deviance ignores) but it's a bit more objective than appealing to social norms. For example, even if a person's sexuality is unusual or shocking to other people, if they can still lead a healthy life then they're not abnormal.
A problem with this is that abnormal behavior may actually be helpful for the individual. For example, taking drugs might help people with stressful jobs or help artists unlock their creativity. In fact, there might be some social groups where not taking drugs is dysfunctional behaviour.
I say "might". They also might kill you. Look at Kurt Cobain! Don't take drugs.
Also, many people engage in behavior that is unhealthy, but we don’t class them as abnormal: adrenaline sports, smoking, drinking alcohol and driving too fast.

|

|

|

|
DISTRESS
This is the simple view that abnormality involves being unhappy: experiencing negative feelings like anxiety, isolation, confusion and fear.

|
Obviously, everyone experiences negative feelings from time to time (exam stress, bereavement, relationship breakup, victims of crime or disasters). However, abnormality is when these negative feelings occur inappropriately or persist longer than they should.
When Prince Albert died in 1861, Queen Victoria went into mourning for the remaining 40 years of her life. She wore black every day and stayed at home for 13 years, refusing even to open Parliament.
|
This has the advantage of connecting abnormality to quality of life, the same as dysfunction (above). You may have odd behaviours like keeping 100 cats in your house, but if it makes you happy, who cares? On the other hand, a phobia of cats is a trivial thing - unless it prevents you from going outside for fear that you will meet one, in which case it is clearly distressing you and must be treated.
A problem with this is that judging distress is quite subjective. It is perfectly normal to be distressed in some situations. After all, who's to say how long you should grieve for after the death of a loved one or the breakup of a relationship? Some people get very distressed about global warming or animal welfare: is that abnormal?
A problem with this is that judging distress is quite subjective. It is perfectly normal to be distressed in some situations. After all, who's to say how long you should grieve for after the death of a loved one or the breakup of a relationship? Some people get very distressed about global warming or animal welfare: is that abnormal?
|
Then there are people who don't feel distress when other people think that they should. If a person stops washing, wearing clean clothes or going outside, most of us would regard that as abnormal and cause for concern.
But if they're perfectly happy being a slobbish couch potato, should they be left to get on with it?
|

|
DANGER
This is when the behaviour harms, or put at risk, the individual or others around them.
This is based on the harm principle, which states that you have a right to behave in any way you like so long as you don't cause harm.
Obviously, there are some things everybody does that can be harmful (like driving a car), but abnormal behaviour puts yourself or other people at excessive risk (like driving a car while drunk).
This is similar to the principle of distress, because it takes a liberal view that people should be left to their own devices if their behaviour is harmless - as opposed to the deviance and dysfunction principles
This is based on the harm principle, which states that you have a right to behave in any way you like so long as you don't cause harm.
Obviously, there are some things everybody does that can be harmful (like driving a car), but abnormal behaviour puts yourself or other people at excessive risk (like driving a car while drunk).
This is similar to the principle of distress, because it takes a liberal view that people should be left to their own devices if their behaviour is harmless - as opposed to the deviance and dysfunction principles
Revise With Rachie has some great videos on A-Level Psychology. Rachie doesn't address the four Ds here but she does describe different ways of defining abnormality

|
APPLYING DIAGNOSES TO REAL LIFE
|
False Positives come from "reading too much" into the client's behaviour. It can also come from the fear of the consequences of a False Negative (if a mentally ill person is told they are normal then goes and hurts or kills themselves). False Negatives can come from the suspicion that the client is faking their illness or the belief that their deviant behaviour is deliberate wickedness. |
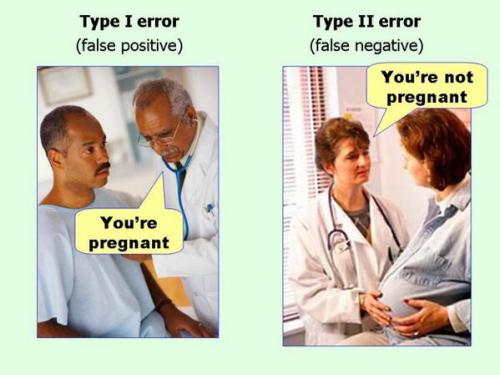
This should keep it clear in your mind.
(It's easy to muddle up Type I and Type II Errors - like Rosenhan did in his study into misdiagnosis) |
|
In the Futurama episode "Insane in the Mainframe", Fry and Bender are sent to the HAL Institute for Criminally Insane Robots (there's a joke in the name - google it).
The story is a joke about Type I and Type II Errors. Bender pretends to be insane by acting like Napoleon but Fry (who isn't a robot at all) goes insane due to the stress of staying there. |
|
When diagnosing schizophrenia using DSM-5, clinicians will look for delusions, hallucinations, disorganized speech and behavior, and other symptoms that show dysfunction. The client must have TWO of these symptoms for a valid diagnosis. In previous editions of DSM, only one symptom was necessary so long as it was "bizarre". So DSM-5 has made False Positives less likely but may have caused False Negatives.
CULTURAL PROBLEMS IN DIAGNOSIS
Psychology is a very Western discipline and psychiatry (the medical study of mental disorders) is very Western in outlook, based on the experiences of doctors and patients in Europe and North America. The DSM is an American diagnositic manual and its influence is huge.
Increasingly, psychiatrists have to diagnose mental disorders in patients from non-Western backgrounds. This might be because Western healthcare is being introduced to non-Western countries (Asia, Africa, South America) or because ethnic minorities in Western countries need mental healthcare.
This matters for several reasons:
Increasingly, psychiatrists have to diagnose mental disorders in patients from non-Western backgrounds. This might be because Western healthcare is being introduced to non-Western countries (Asia, Africa, South America) or because ethnic minorities in Western countries need mental healthcare.
This matters for several reasons:
- Disorders, classifications and symptoms that are recognised by Western psychiatry become "official" mental disorders and attract research which develops treatments; "unofficial" mental disorders are considered to be folk illnesses and are not taken seriously. This can lead to false negative diagnosis.
- People from other cultures presenting their symptoms to a Western doctor may express themselves in unfamiliar ways. For example, among African-Caribbeans it is not abnormal to talk to dead relatives while grieving. This can lead to them being diagnosed with a much more severe disorder than they really have (such as schizophrenia rather than mild depression) - a false positive diagnosis.
'MEDICALISING' NORMAL EXPERIENCES
Related to False Positives is the concern that clinical psychologists are 'medicalising' normal experiences like sadness, anger, laziness and bad habits. This means that feelings that used to be seen as normal parts of life and behaviours that used to be viewed as down to willpower and conscience are now seen as medical problems instead.
Lisa Appignanesi (2008) argues there are a number of reasons for this:
The latest edition of DSM has been criticised for this, because it contains a lot of "new" mental disorders that include shyness and loneliness as well as unhappiness over bereavement.
Critics like psychiatrist Nick Craddock argue that if people believe they have a mental illness when in fact they are going through a normal experience, this does more harm than good.
Lisa Appignanesi (2008) argues there are a number of reasons for this:
- We trust doctors and accept a medical diagnosis more than people in the past did
- Doctors want to help and believe that, if our problems are medical in nature, then they can be treated
- We are lazy and believe that, if our problems are medical in nature, it's up to doctors to fix them, not us to change or improve
- Companies that make medicines ('Big Pharma') want to sell us their cures. even if the medical problem doesn't really exist
The latest edition of DSM has been criticised for this, because it contains a lot of "new" mental disorders that include shyness and loneliness as well as unhappiness over bereavement.
Critics like psychiatrist Nick Craddock argue that if people believe they have a mental illness when in fact they are going through a normal experience, this does more harm than good.
Somebody who is bereaved might need help and even counselling, but they did not need a label saying they had a mental illness - Nick Craddock
Some clinical psychologists defend this trend. They argue that, by medicalising problems, we focus on treatment rather than blame. Medicalising problems also removes a lot of stigma from behaviours that people used to be ashamed of and keep secret, making it more likely they will come forward and seek help.
|
A famous example of medicalising normal experience might be oppositional-defiant disorder which appeared back in DSM-III (1980). This is a disorder among children that makes them argumentative and disobedient toward their parents.
Critics say it used to be known as "naughtiness" before it was medicalised. |
|
|
EVALUATING DIAGNOSES
|
|
Even if we don't agree with the recovery model, it still makes some good points. People with mental disorders are more than just broken machines that need to be "fixed" by a wonder-drug. Medical diagnoses can become part of the problem, taking away people's sense of control over themselves, making them see themselves as a damaged human beings; they become dependent on drugs and psychiatrists to make their life bearable rather than trying to change their life.
|
|
Applications
Timothy Davis (2009) argues that diagnosing mental disorders involves deciding when a characteristic is problematic enough to become a clinical diagnosis. The four Ds can assist in making a decision by matching behaviour and beliefs to the DSM. This helps therapists to know when a condition might need a DSM diagnosis,
Diagnoses are conducted through clinical interviews. These are semi-structured interviews which gather information on the client's behaviour to make a clinical assessment. This could lead to problems because semi-structured interviews can be unreliable, subjective and biased. For example, African-Caribbean people in the UK are 3-5 times more likely to be diagnosed with schizophrenia and hospitalised than other groups. You are also more likely to be diagnosed with serious mental disorders if you are poor. Women are more likely to be diagnosed than men.
Timothy Davis (2009) argues that diagnosing mental disorders involves deciding when a characteristic is problematic enough to become a clinical diagnosis. The four Ds can assist in making a decision by matching behaviour and beliefs to the DSM. This helps therapists to know when a condition might need a DSM diagnosis,
Diagnoses are conducted through clinical interviews. These are semi-structured interviews which gather information on the client's behaviour to make a clinical assessment. This could lead to problems because semi-structured interviews can be unreliable, subjective and biased. For example, African-Caribbean people in the UK are 3-5 times more likely to be diagnosed with schizophrenia and hospitalised than other groups. You are also more likely to be diagnosed with serious mental disorders if you are poor. Women are more likely to be diagnosed than men.
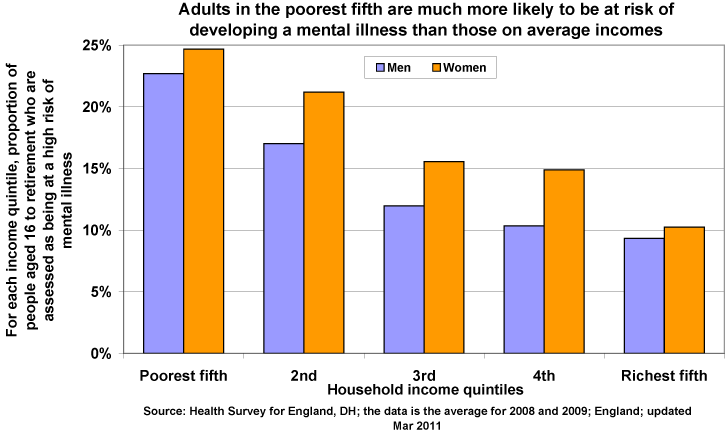
What's not clear is whether people from poorer backgrounds really do suffer more from mental illness (due to stress and unhappiness) or whether these are Type I Errors by doctors who aren't very sympathetic towards them. Are women more ill than men or are they just more willing to report embarrassing emotional problems like depression and hallucinations?
|
Labeling someone as abnormal using the four Ds might be used to force people to conform to the society's standards. If they do not, then psychiatric treatment will 'normalise' their behaviour. This is a form of social control that can become oppressive and unjust.
In the '60s and '70s, the Soviet Union was condemned for declaring political opponents to be "mad" and putting them in mental asylums (psikhushkas). Wanting to have democratic freedom was considered a symptom of paranoid schizophrenia. Vladimir Burosky is a famous Russian activist who experienced this himself. |

A psikhushka (mental asylum) where Vladimir Burosky was imprisoned for his beliefs - an extreme example of Type I Errors at work
|
|
EXEMPLAR ESSAY
|