

|
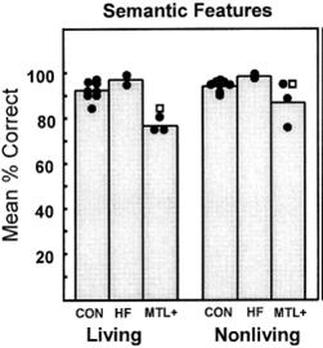
As a Contemporary Study, this study is one of three (the others are Steyvers & Hemmer and Sebastián & Hernández-Gil). This means the Examiner doesn't know which Contemporary Study you will have covered - so there will never be a question specifically on Schmolck et al. You won't get asked what "MTL+" means or how the controls scored in the category sorting task. However, you will get general questions about the Aim, Procedure, Results and Conclusions (APRC) of the Contemporary Study and you may be asked to evaluate it in terms of Generalisability, Reliability, Applications, Validity or (possibly) Ethics (GRAVE).
|

|
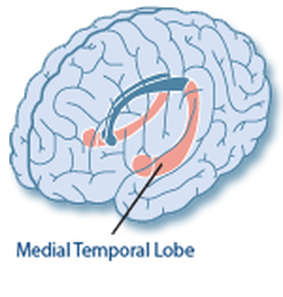
SCHMOLCK ET AL. (2002)
|

|
SCHMOLCK ET AL.'S STUDY
|
|
EVALUATING SCHMOLCK ET AL. AO3
|
|
EXEMPLAR ESSAY
|