
|
PSYCHOLOGICAL TREATMENTS FOR SCHIZOPHRENIA
The Edexcel course requires you to know about one psychologically-based treatment for schizophrenia. You will need to be able to compare this with a biological treatment.
There are other psychological treatments besides CBT. For example, there is psychoanalysis (Freud's "talking cure") and behavioural therapy (like token economy programmes) but these are less commonly used and more controversial. Some students who enjoyed Freud in Unit 1 might prefer to write about Freud's psychoanalysis as a psychological treatment for schizophrenia. I've included some sections on this that other students may ignore.
|
|
COGNITIVE BEHAVIOURAL THERAPY FOR SCHIZOPHRENIA
|
|
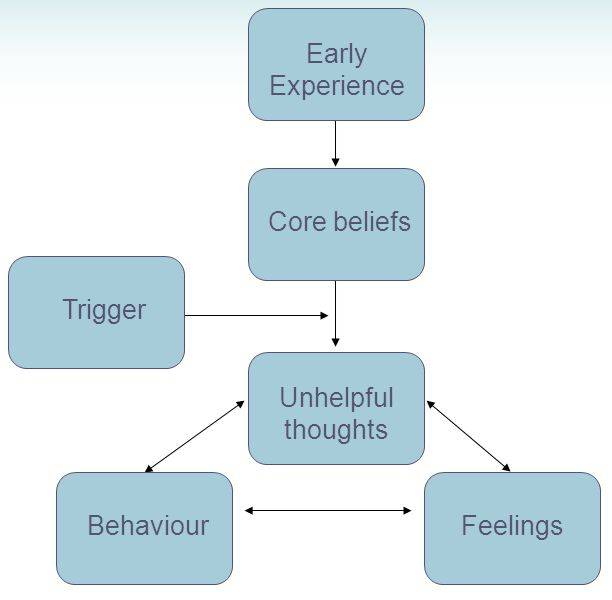
Beck proposed the Cognitive Triad. This is the idea that our thoughts and beliefs shape our feelings and our feelings then direct the way we behave; our behaviour then influences the way other people treat us and that in turn backs up our thoughts and beliefs.
Beck suggests a lot of behavioural problems stem from "faulty thinking" - core beliefs that are negative and irrational. For example, if a person thinks that people don't like them, they will feel bitter and upset. If they feel this way, they will act defensively and be aloof and cold. If they behave this way, people won't like them... |

The Cognitive Triad is an example of a VICIOUS CIRCLE. Beck's therapy was an attempt to re-wind the negative process and create a 'virtuous circle'.
|
Beck's cognitive therapy was a gentle process, getting clients to question their core beliefs. Albert Ellis' Rational Emotive Behavioural Therapy (REBT) was more aggressive. Ellis believed faulty thinking should be challenged and exposed for what it was. Ellis proposed the A-B-C Model of behavioural change:
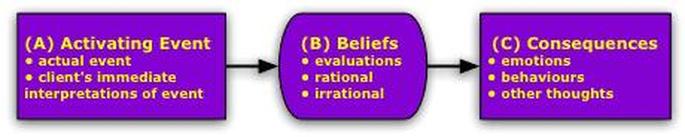
The therapist gets the client to identify an "activating event" - something they believe is the trigger for their problems. For someone with schizophrenia, this might be a delusion or a hallucination. The client then identifies their "beliefs" about this event. People with schizophrenia often think the voices they hear are real. Therapist and client then explore the "consequences" of these beliefs, such as how talking back to the voices upsets and frightens other people around them.
|
Ellis also proposed a fourth step - D for "dispute" - in which the therapist challenges the client's beliefs, exposes them as faulty and gets the client to adopt different beliefs (for example, that the voices are "just in their head").
It's important that the "D" part is non-judgmental. The therapist isn't trying to make the client feel bad for having these beliefs.
|
|
|
Cognitive Behavioural Therapy (CBT) combines Beck's and Ellis' therapies. A CBT therapist encourages the client to become aware of their own core beliefs, which may have been formed by unpleasant early experiences.
They then work out what sort of events act as triggers for unhelpful thoughts. Therapist and client decide decide how to put these beliefs to the test, perhaps through role-playing what happens when they act on their unhelpful thoughts compared to when they act on more positive thoughts. |
7-minute video outlining how CBT treats schizophrenia
Many people with schizophrenia have their own (often ineffective) coping strategies to control their delusions and hallucinations, so CBT improves these coping strategies (Nicholas Tarrier, 1987).
CBT for schizophrenia focuses on the positive symptoms (hallucinations and delusions) rather than the negative symptoms (such as lack of emotion, lack of motivation, speaking very little). Coping Strategy Enhancement works by figuring out the triggers for delusions and hallucinations and the coping strategies the client uses. The therapist and client work together to improve the existing coping strategies. The patient is given “homework” of putting the new strategies into action. In the next session, therapist and client review how this went and discuss ways of making these strategies more effective.
CBT also focuses on changing the client's delusions and hallucinations. The client is asked to think of explanations for his or her beliefs. After this, there is “reality testing”, in which the therapist and client plan an activity to put a delusional belief to the test. For example, if the client thought they had a special power the therapist would ask them to demonstrate it.
CBT for schizophrenia focuses on the positive symptoms (hallucinations and delusions) rather than the negative symptoms (such as lack of emotion, lack of motivation, speaking very little). Coping Strategy Enhancement works by figuring out the triggers for delusions and hallucinations and the coping strategies the client uses. The therapist and client work together to improve the existing coping strategies. The patient is given “homework” of putting the new strategies into action. In the next session, therapist and client review how this went and discuss ways of making these strategies more effective.
CBT also focuses on changing the client's delusions and hallucinations. The client is asked to think of explanations for his or her beliefs. After this, there is “reality testing”, in which the therapist and client plan an activity to put a delusional belief to the test. For example, if the client thought they had a special power the therapist would ask them to demonstrate it.
WHAT ABOUT PSYCHOANALYSIS?
Psychoanalysis is the original "talking cure" that inspired Aaron Beck. It also involves one-to-one session with a therapist (called a psychoanalyst).
Unlike CBT, psychoanalysis focuses on unconscious feelings and desires. Because the client cannot know their own unconscious mind, there's no point in the sort of activities that CBT involves. Instead, the analyst has to help the client understand his or her unconscious. This is done through activities like dream analysis, free association or the Rorschach inkblot test.
The assumption in psychoanalysis is that the client's problems stem from childhood trauma - probably a traumatic relationship with a parent. There may be memories of childhood abuse that the client has repressed. The client's abnormal behaviour is in fact a defence mechanism to avoid facing these memories. The traumatic memories must be brought into the conscious mind and confronted so that the defence mechanisms are no longer needed.
Unlike CBT, psychoanalysis focuses on unconscious feelings and desires. Because the client cannot know their own unconscious mind, there's no point in the sort of activities that CBT involves. Instead, the analyst has to help the client understand his or her unconscious. This is done through activities like dream analysis, free association or the Rorschach inkblot test.
The assumption in psychoanalysis is that the client's problems stem from childhood trauma - probably a traumatic relationship with a parent. There may be memories of childhood abuse that the client has repressed. The client's abnormal behaviour is in fact a defence mechanism to avoid facing these memories. The traumatic memories must be brought into the conscious mind and confronted so that the defence mechanisms are no longer needed.

|
APPLYING CBT TO REAL LIFE
|
|
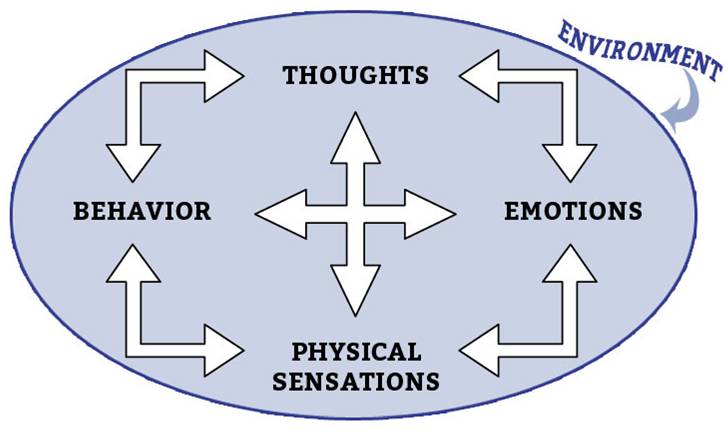
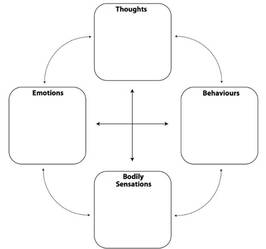
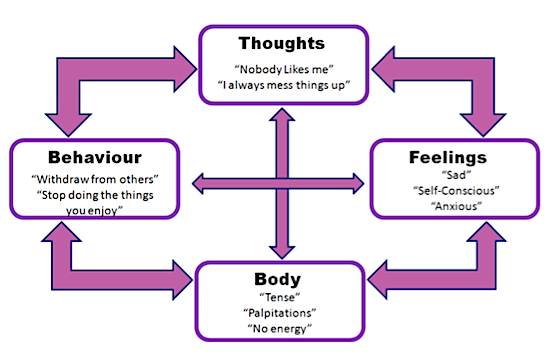
A technique often used in CBT is the "Hot Cross Bun" (Padesky & Mooney, 1990), which adds the importance of "physical sensations" alongside thoughts, emotions and behaviour. Physical sensations can be easier to recognise and talk about than thoughts or feelings.
This is particularly useful for clients with schizophrenia, who can experience intense physical sensations. |
|
|
|
"Homework" for a CBT session might involve identifying situations where unpleasant physical sensations happen, then filling in the 'hot cross bun' template (above). The client and therapist will 'work back' through behaviour/feelings to arrive at the core beliefs which are causing the problem. The next CBT session can focus on these beliefs.
|
3-minute overview of how CBT works
|
Excellent 3-minute video illustrating how CBT helps people with schizophrenia
|
APPLYING & EVALUATING PSYCHOANALYSIS
Freud believed that schizophrenics were unable to develop the close interpersonal relationship with the therapist necessary for psychoanalysis.
Harry Stack Sullivan (1892-1949) adapted Freud's ideas. He suggested that a person with schizophrenia has a very fragile ego and has regressed to early childhood due to extreme stress. Therapy gets the client to achieve insight in to role that the past has played in current problems. This has been referred to as an ego-analytical approach.
Harry Stack Sullivan (1892-1949) adapted Freud's ideas. He suggested that a person with schizophrenia has a very fragile ego and has regressed to early childhood due to extreme stress. Therapy gets the client to achieve insight in to role that the past has played in current problems. This has been referred to as an ego-analytical approach.
Great success was claimed by Sullivan (from the 1920s). However, Sullivan's patients were only mildly disturbed and may not have been diagnosed as schizophrenic using DSM criteria.
Stone (1986) shows half of the sample of more than 500 schizophrenic patients discharged after treatment between 1963 and 1976 in New York were doing poorly. Stone suggests that psychoanalytic 'insight' may worsen the condition by making people focus on problems in their past they can do nothing about.
However, Rosenbaum et al. (2012) compared people with schizophrenia being treated with psychoanalysis with those being given conventional treatment over two years; the psychoanalysis group improved far more than the control group, improving their social functioning and showing decreases in symptoms.
Stone (1986) shows half of the sample of more than 500 schizophrenic patients discharged after treatment between 1963 and 1976 in New York were doing poorly. Stone suggests that psychoanalytic 'insight' may worsen the condition by making people focus on problems in their past they can do nothing about.
However, Rosenbaum et al. (2012) compared people with schizophrenia being treated with psychoanalysis with those being given conventional treatment over two years; the psychoanalysis group improved far more than the control group, improving their social functioning and showing decreases in symptoms.
|
EVALUATING CBT
|

|
EXEMPLAR ESSAY
|