

|
You don't need to know everything on this page. The Exam will only ask you about non-biological explanations for "a disorder other than schizophrenia" - it won't ask specifically about depression or cognitive explanations. However, you should be able to explain at least one of these factors in depression and evaluate them. Material from psychological treatments for depression is helpful for evaluating this explanation as well.
|

|
NON-BIOLOGICAL EXPLANATIONS OF DEPRESSION
The Unit 2 Exam expects you to know about one non-biological explanation of a disorder other than schizophrenia; in this case, unipolar depression.
You are also expected to understand a psychological treatment for depression which is linked to these explanations. WHAT ABOUT FREUD?
In Unit 1, students had to learn about Freud's psychodynamic theory and his views on aggression, development and individual differences. Some students might prefer to make use of this material here, as an alternative explanation of depression.
|
|
DEPRESSION & FAULTY COGNITIONS
|
|
HeSeligman & Maier (1967) was a bombshell study because it brought Behaviourism (a philosophy based on Learning Theory) crashing down. The dogs demonstrated that there are such things as cognitions - in this case, feelings of helplessness - which influence behaviour more than external stimuli.
By the way, Seligman wasn't always a guy in a suit. In the '60s and '70s, he looked a bit different. He was also one of Rosenhan's pseudopatients. |
Best. Decade. Ever.
|
Seligman went on to link learned helplessness to depression in humans. He suggested that people have an "explanatory style" - their way of making sense of what happens to them. People with a pessimistic explanatory style see negative events as:
- stable ("it will always be like this")
- global ("everything else will be like this too")
- internal ("it's my fault that it's like this")
Seligman argued that explanatory style was learned through upbringing, but that a different and more optimistic explanatory style could be learned through cognitive therapy. An optimistic explanatory style sees negative events as:
- unstable ("this too will pass")
- specific ("other things aren't like this")
- external ("this happens to everyone, it's not just me")
Learned helplessness is also linked to brain function. Hammack et al. (2011) showed that serotonin is linked to feelings of helplessness as well as activity in the amygdala. Serotonin and the amygdala are known to be linked to depression as well.

|
Another psychologist investigating the cognitive side of depression was Aaron Beck (right).
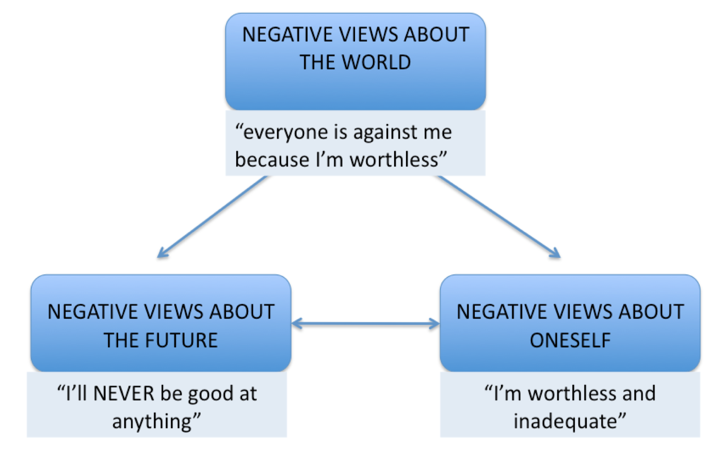
Beck proposed three cognitive factors in depression:
|
|
|
Beck's negative cognitive triad is the idea that people have negative views about the world that influence their feelings about themselves and their expectations of the future. Negative views about oneself and the future feed back into a negative worldview. People then act on these feelings, usually by giving up on projects, withdrawing from relationships and blaming themselves. This destructive behaviour causes them to fail at things and struggle in relationships, which convinces them that their core beliefs are right.
|
|
This sort of thing is called a VICIOUS CIRCLE.
A particularly charming portrayal of negative thinking is "Marvin the Android" from Douglas Adams' The Hitch Hikers Guide to the Galaxy (1978). Here he is in the 2005 film version, voiced by the late great Alan Rickman. |
|
Beck also identifies errors in logic, called cognitive biases, in people with depression:
Polarised thinking is another bias, also known as black-and-white thinking. For example, people with depression often set themselves unattainable standards such as, “I must be liked by everybody; if not, I’m a terrible person” or "I must succeed at everything; if not, I'm completely useless".
- magnification: problems are exaggerated
- minimisation: strengths and opportunities are under-emphasised
- personalisation: the individual blames themselves for things that are actually beyond their control
Polarised thinking is another bias, also known as black-and-white thinking. For example, people with depression often set themselves unattainable standards such as, “I must be liked by everybody; if not, I’m a terrible person” or "I must succeed at everything; if not, I'm completely useless".
Negative schemas develop during childhood, usually through critical relationships (like parents who are too perfectionist or school cliques that are judgmental) or traumatic events (like the death of a family member, childhood abuse or bullying at school). They are activated when the person experiences similar situations or similar relationships in later life.
You came across SCHEMAS back when you were studying the reconstructive theory of memory. There, schemas were stereotypes that affected how we remember the past; here, they also affect what we expect from the future and how we think we are expected to react to things. They're like the "unwritten rules" of your life. Beck's "schemas" and Seligman's "explanatory styles" seem to be the same thing.
This 5-minute podcast sums up cognitive views of depression - with a bit on CBT as well
FREUD'S PSYCHODYNAMIC EXPLANATION
In Unit 1, you studied Freud as an alternative to the biological explanation of aggression. You could use his ideas again as an alternative to biological explanations of depression.
According to Freud's psychodynamic approach, abnormality is caused when trauma from unresolved conflict between the id, ego, and superego is repressed into the unconscious. Freud believed that in people with depression the superego (or conscience) is over-developed. This explains the excessive guilt and the sense of worthlessness people with depression feel.
This imbalance can be caused by fixation or regression to an earlier stage of psychosexual development. Freud argued that, if your needs weren’t met during the oral stage, you develop low self-esteem and excessive dependence ("neediness") which puts you at risk of depression in adulthood.
On the other hand, if your needs were met to excess during the oral stage, you might also might become too dependent on others.
This imbalance can be caused by fixation or regression to an earlier stage of psychosexual development. Freud argued that, if your needs weren’t met during the oral stage, you develop low self-esteem and excessive dependence ("neediness") which puts you at risk of depression in adulthood.
On the other hand, if your needs were met to excess during the oral stage, you might also might become too dependent on others.
|
It might seem like you just can't win with Freud! But Freud's idea is that psychological health is a precarious balancing act. Too little parental love and support stunts our growth - but so does smothering.
Remember Goldilocks and the porridge? Your childhood relationships need to be not too hot, not too cold, but "just right". |

|
People who are excessively dependent on others are particularly likely to develop depression after a loss. This could be a bereavement or the breakup of a relationship, losing a job or falling out with a friend. Anger at the loss is displaced, causing you to re-experience a painful loss that occurred in childhood.

|
APPLYING NON-BIOLOGICAL EXPLANATIONS OF DEPRESSION
| ||||||
|
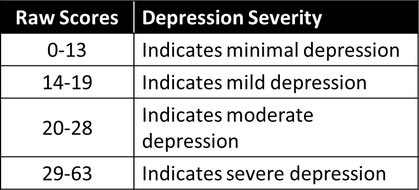
Beck also created the Beck Depression Inventory (BDI) in 1961. This is a 21-question psychometric test that asks about cognitions (hopelessness, irritability, guilt or feelings of being punished) as well as physical symptoms such as fatigue, weight loss, and lack of interest in sex. Each question is multiple-choice, with 4 answers to choose from. These are rated 0 to 3 and the overall score is out of 63.
|
|
|
| ||
BDI is often used to measure the severity of depression and to check how a client is responding to treatment. It's not meant to be a diagnostic tool however so it shouldn't replace visiting your doctor if you think you might be depressed.
The contemporary study in depression by Kroenke et al. introduces a new questionnaire for measuring depression: the PHQ-8. This is also based on a cognitive understanding of depression, asking questions about feeling down, feeling like a failure and inability to concentrate.
APPLYING THE PSYCHODYNAMIC EXPLANATION
Freud was the psychologist who pioneered the idea of the "talking cure" which he called psychoanalysis. However, psychoanalysis is different from normal cognitive therapy.
The psychodynamic explanation suggests that the causes of schizophrenia are buried in the unconscious mind, in memories of a distressing childhood. The client has created the symptoms of depression to protect themselves from these memories. So there's no point in just asking the client for their opinion about their illness.
Instead, the psychoanalyst tries to guide the client towards insight and self-knowledge. This might involve techniques like free association or the Rorschach inkblot test.
The psychodynamic explanation suggests that the causes of schizophrenia are buried in the unconscious mind, in memories of a distressing childhood. The client has created the symptoms of depression to protect themselves from these memories. So there's no point in just asking the client for their opinion about their illness.
Instead, the psychoanalyst tries to guide the client towards insight and self-knowledge. This might involve techniques like free association or the Rorschach inkblot test.
|
EVALUATING NON-BIOLOGICAL EXPLANATIONS
|
With only 8 marks for AO1, don't waste time with describing cognitive explanations
Just start with an evaluation point and use evidence to back it up.
You can add in extra knowledge to develop an argument.
More purple (AO3) than blue (AO1) is a good sign.
An AO3 point with AO1 backup is a "logical chain of reasoning"
Evaluation point + evidence + counterpoint is another good structure
For a top band answer, address factors (plural) not just one factor - eg. Freud or behaviourism (conditioning, role models)
The integrated approach or the diathesis-stress model make great conclusions
|
EXEMPLAR ESSAY
|
- Notice that for a 20-mark answer you don’t have to include everything about the cognitive explanation of depression. Here, all the description appears as evidence in support of an evaluation point. The AO1 description is blue and the AO3 evaluation is purple. You can see there's more purple than blue in this essay - because there are 12 AO3 marks but only 8 AO1.
- About 6 paragraphs like this, each with a mix of AO1 and AO3, should be enough, plus the conclusion of course. If you aim for the top band, add 2 more paragraphs considering other factors than just cognitivism.