

|
You need to be able to describe, evaluate and compare TWO biological explanations of schizophrenia. One of them MUST be the functioning of neurotransmitters (the "Dopamine Hypothesis"), so you need to know this in detail and the Exam could ask your specifically about neurotransmitters. The Specification also mentions genes and mental health, so the second explanation here is a genetic one. You could be asked for "a biological explanation of schizophrenia OTHER THAN NEUROTRANSMITTERS" or "how genes affect mental health" (with specifying schizophrenia).
|
|
NON-BIOLOGICAL EXPLANATIONS FOR SCHIZOPHRENIA
The Unit 2 Exam expects you to know about one non-biological explanation of schizophrenia. This page with consider cognitive explanations and Freudian (psychodynamic) explanations.
You are also expected to understand a psychological treatment for schizophrenia which is linked to this explanation. As part of Clinical Psychology, you will look at Bradshaw's case study of Carol, which claims that there is a cognitive aspect to schizophrenia and that the disorder can be treated with counseling.
In this 15 minute video, Eleanor Longden describes her voices and therapy from a cognitive perspective (and the Recovery Model)
WHAT ABOUT FREUD?
In Unit 1, students had to learn about Freud's psychodynamic theory and his views on aggression, development and individual differences. Some students might prefer to make use of this material here, as an alternative explanation of schizophrenia.
|

|
SCHIZOPHRENIA & FAULTY COGNITIONS
|
|
Cognitive deficits are a key symptom of schizophrenia. However, 'faulty cognitions' might be responsible for a lot of the negative and positive symptoms of schizophrenia too. Faulty cognitions include poor attention and memory, difficulties with language and disorganised thinking.
One of the most important cognitive theories of schizophrenia is attention deficit theory.
Christopher Frith (1979) argues schizophrenia is the result of a faulty attention system. |

|
|
Preconscious thought (thought that occurs without awareness) contains a huge amount of information from our senses that would normally be filtered. If this filtering process doesn't happen, there will be sensory overload. Thoughts that would usually be filtered out as irrelevant or unimportant are noticed instead and treated as more significant than they really are. Frith says this accounts for the positive symptoms of schizophrenia, such as hallucinations, delusions and disorganised speech.
|
David Hemsley (1993, 2005) suggests schizophrenia involves a breakdown in the relationship between memory and perception. People with schizophrenia have a disconnect between their schemas (expectations of certain situations) and what they actually hear and see. When they encounter new situations, their schemas are not activated. As a result, people with schizophrenia experience sensory overload because they do not know which aspects of a situation to attend to and which to ignore. It also means they struggle to predict what will happen next. Their poor integration of memory and perception leads to disorganised thinking and behaviour.
Schizophrenic symptoms boil down to a lack of self-monitoring; thoughts and ideas are attributed to external sources (such as hallucinations), or result in delusions because the individual does not realise that they are self-generated. They mistakenly regard their own thoughts as alien and coming from someone else. PET scans of people with schizophrenia show under-activity in the frontal lobe of the brain, which is linked to self-monitoring.
Schizophrenic symptoms boil down to a lack of self-monitoring; thoughts and ideas are attributed to external sources (such as hallucinations), or result in delusions because the individual does not realise that they are self-generated. They mistakenly regard their own thoughts as alien and coming from someone else. PET scans of people with schizophrenia show under-activity in the frontal lobe of the brain, which is linked to self-monitoring.
The "schizophrenia simulator" gives a vivid insight into the consequences of problems with attention
FREUD'S PSYCHODYNAMIC EXPLANATION
In Unit 1, you studied Freud as an alternative to the biological explanation of aggression. You could use his ideas again as an alternative to biological explanations of schizophrenia.
According to Freud's psychodynamic approach, abnormality is caused when trauma from unresolved conflict between the id, ego, and superego is repressed into the unconscious. This causes fixation or regression to an earlier stage of psychosexual development. If the ego is not fully developed, the individual may be dominated by the id or the superego, and will lack a sound basis in reality.
This might happen if someone experienced a very harsh childhood, perhaps because their parents were cold and unsupportive. The child becomes fixated or regresses to an earlier stage of development that was safer or more comforting.
Schizophrenia is linked to the oral stage; in particular, a stage called primary narcissism during which the ego has not separated from the id. Because the ego is the rational part of the mind, if you regress to a stage before it forms. you will stop operating on the reality principle and lose touch with reality. This explains some of the symptoms of schizophrenia, especially hallucinations, delusions and disorganized thought and speech.
This might happen if someone experienced a very harsh childhood, perhaps because their parents were cold and unsupportive. The child becomes fixated or regresses to an earlier stage of development that was safer or more comforting.
Schizophrenia is linked to the oral stage; in particular, a stage called primary narcissism during which the ego has not separated from the id. Because the ego is the rational part of the mind, if you regress to a stage before it forms. you will stop operating on the reality principle and lose touch with reality. This explains some of the symptoms of schizophrenia, especially hallucinations, delusions and disorganized thought and speech.
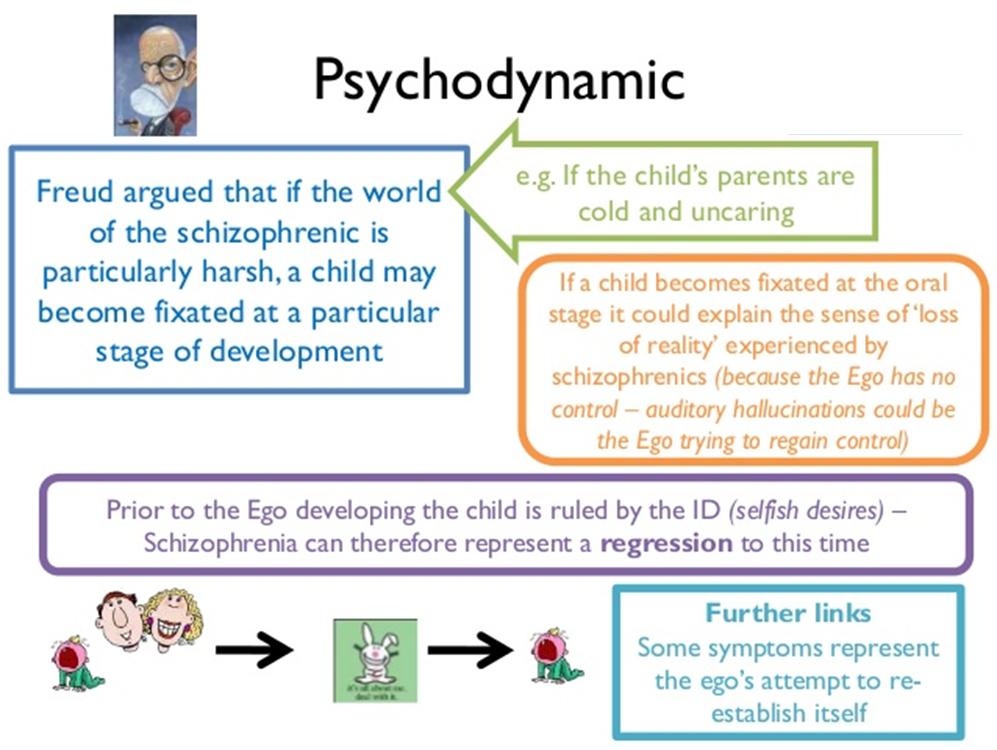
Freud's view boils down to the idea that, in the face of fear and loneliness, a child retreats into itself, living in "a world of its own" because they find the outside world too threatening.

|
APPLYING FAULTY COGNITIONS TO REAL LIFE
|
|
EVALUATING COGNITIVE EXPLANATIONS
|

|
EXEMPLAR ESSAY
|