

|
CARLSSON ET AL. (2000)
|
|
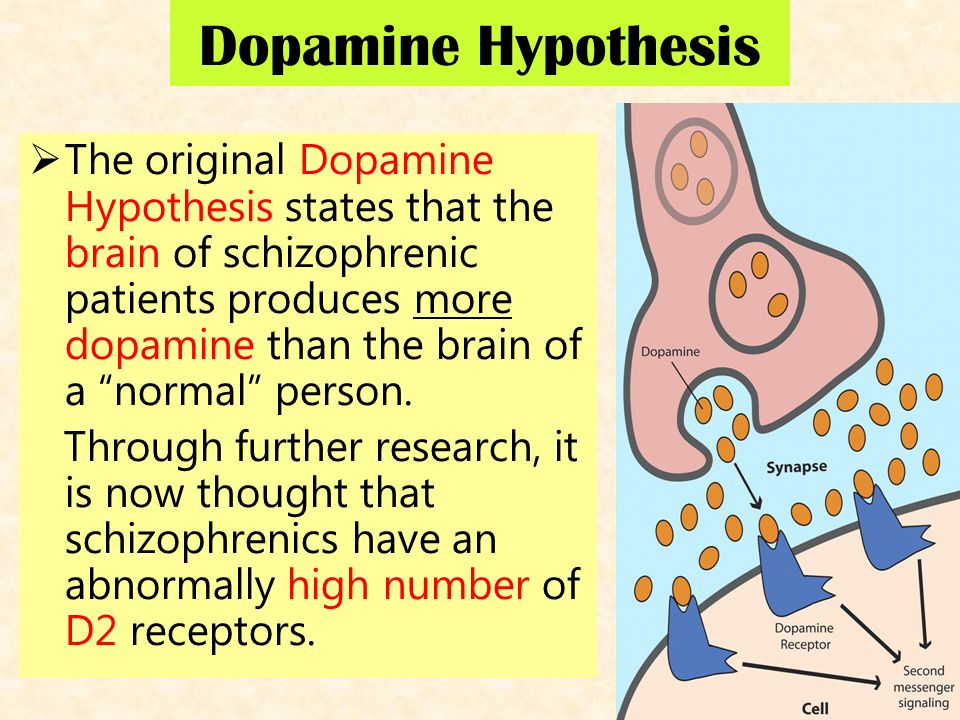
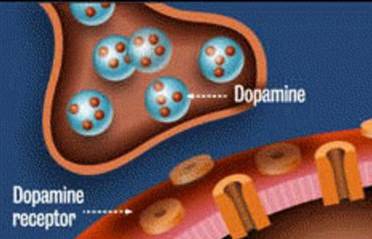
Neurotransmitters are "fast chemical messengers" that travel between neurons (brain cells) by crossing the synapse. They bind themselves to receptors on the next neuron and pass in their message in the form of a small electric charge.
Dopamine is an important neurotransmitter that regulates mood and attention. It seems to be linked to schizophrenia in a number of ways. The Dopamine Hypothesis was proposed by Arvid Carlsson and suggests that schizophrenia is caused by too much dopamine - or too many dopamine receptors - in key areas of the brain. |
|
Carlsson refers to the Dopamine Hypothesis as the theory of "dopaminergic dysfunction". He also refers to "hyperdopaminergia" and "hypodopaminergia".

|
"Dopaminergic" means "related to dopamine". "Hyper" means "overactive" and "hypo" means "underactive" - so HYPERdopaminergia is a condition of having too much dopamine activity and HYPOdopaminergia is having too little.
|
WHAT IS GLUTAMATE?
Glutamate is an unusual chemical that does a lot of things (for example, it's used as a food additive). It took a long time for scientists to realise that it also worked as a neurotransmitter.
Glutamate is present in high quantities throughout the brain. In very high quantities it is toxic, but the majority (99.9%) of glutamate is stored inside brain cells. Glutamate only works as a neurotransmitter when it is outside brain cells. Chemicals called glutamate transporters "uptake" loose molecules of glutamate, binding them safely inside cells.
Glutamate is present in high quantities throughout the brain. In very high quantities it is toxic, but the majority (99.9%) of glutamate is stored inside brain cells. Glutamate only works as a neurotransmitter when it is outside brain cells. Chemicals called glutamate transporters "uptake" loose molecules of glutamate, binding them safely inside cells.
|
Glutamate uptake is an example of one of those processes that keeps brain chemistry "just right" - like Goldilocks' porridge. Levels of glutamate outside the brain cells mustn't be too high (hyperglutamatergia) or too low (hypoglutamatergia).
|

|
As a neurotransmitter, glutamate controls memory and learning by binding to glutamate receptors (for example, NMDA is a common glutamate receptor). These receptors are found everywhere in the brain, which is why it's important for glutamate levels to be kept low by healthy glutamate uptake.

|
CARLSSON ET AL.'S STUDY
|
|
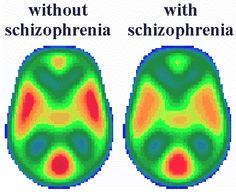
Some PET tracers are designed to bind to receptors on neurons in the brain. They won't be able to do this if certain neurotransmitters are over-active in the brain. Therefore, on a PET scan, these areas will show up as lacking in radioactivity, coloured green or blue. On the other hand, if these neurotransmitters are under-active in the brain, the tracers will bind themselves to lots of receptors and show up on the PET scan as yellow and red areas.
|
|
Carlsson also mentions SPECT scans. SPECT scans are cheaper but less accurate versions of PET scans that use gamma rays instead of positrons.
Results
As a review study, this paper mostly consists of 'results'. However, most of these results aren't from Carlsson's research - although some are - but from other researchers that get cited.
Carlsson's review is set out in 7 sections. I'll present key ideas and a piece of research for each section, but students don't need to know all of them - just a couple should be enough if you also know Aims, Procedures and/or Conclusions.
Carlsson's review is set out in 7 sections. I'll present key ideas and a piece of research for each section, but students don't need to know all of them - just a couple should be enough if you also know Aims, Procedures and/or Conclusions.
1 |
Introduction - the dopamine hypothesis revisited
|
Carlsson explains evidence from PET/SPECT that supports the Dopamine Hypothesis (dopaminergic dysfunction):
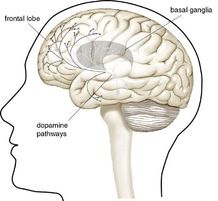
- Schizophrenic participants show more dopamine activity than a healthy control group, especially in a part of the brain called the basal ganglia
- However, Laruelle et al. (1999) found that schizophrenia patients in remission (not showing symptoms) only had normal dopamine activity
- Carlsson et al. point out the patients taking antipsychotics complain most about the side-effects while their symptoms are in remission - not surprising if their dopamine activity becomes normal during this time and the drugs are causing hypodopaminergia (too little dopamine)
2 |
Beyond dopamine
|
Neurotransmitters interact and affect each other, so is dopamine the only neurotransmitter at work in schizophrenic symptoms? Carlsson et al. focus on glutamate for two reasons:
- Drugs like PCP ("angel dust") and ketamine produce psychotic symptoms, but instead of activating dopamine they stimulate glutamate receptors called NMDA
- Lodge et al. (1989) claim glutamate activity at NMDA receptors produces psychotic reactions (it is "psychotogenic") in rats and humans
3 |
Glutamatergic control of dopamine release
|
Glutamate seems to regulate the behaviour of dopamine and sheds some light on the behaviour of dopamine in the brain. Carlsson describes how it acts as an "accelerator" (increasing dopamine activity) or a "brake" (decreasing it).
- Miller & Abercrombie (1996) show that the release of dopamine is increased if glutamate activity is reduced (by blocking the NMDA receptors which glutamate binds with)
- The psychotic side-effects of PCP are reduced by a chemical called LY354740, which increases the activity of glutamate but doesn't do anything directly to dopamine (this suggests that high glutamate activity has the effect of inhibiting dopamine).
4
|
Glutamate-dopamine interaction at the postsynaptic (striatal) level
|
|
Low levels of glutamate (hypoglutamatergia) seems to link with both positive and negative schizophrenic symptoms. Carlsson locates this activity in an area of the brain called the striatum (in the basal ganglia) and in the cerebral cortex (which includes the frontal lobe, where conscious behaviour happens).
|
|
- The striatum (basal ganglia) is the brain's reward centre, so abnormal activity there will lead to the positive symptoms of schizophrenia
- Low glutamate activity in the NMDA receptors in the cerebral cortex would explain the negative symptoms of schizophrenia
glutamatergic failure in the cerebral cortex may lead to negative symptoms, whereas glutamatergic failure in the basal ganglia could be responsible for the positive symptoms - Arvid Carlsson
5
|
The thalamic filter
|
|
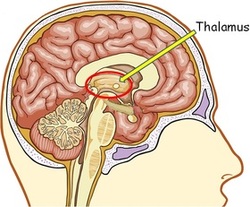
Carlsson has his own theory about what's going on. The thalamus is an important brain structure between the stratium and the cerebral cortex. Carlsson proposes that the thalamus "filters off" neurortransmitters coming out of the stratium to stop the cerebral cortex from overloading. There are two "pathways" through the thalamus:
|
|
- In the indirect pathway, too much dopamine (hyperdopaminergia) or too little glutamate (hypoglutamatergia) reduces the "protective influence" of the thalamus - this links to positive symptoms
- There's also a direct pathway, which has the opposite effect; abnormal dopamine and glutamate activity here will "excite" the thalamus, starving the cerebral cortex of stimulation - this links to negative symptoms
6
|
Comparing two experimental schizophrenia models - therapeutic implications
|
This leaves us with two models (explanations) for schizophrenia: hyperdopaminergia (too much dopamine) or hypoglutamatergia (too little glutamate).
- Some patients respond better to some drugs than others and this might be because some people's schizophrenia is more dopaminergic and other people's symptoms are more glutamatergic
- The "treatment resistant" patients who don't respond to typical antipsychotics (that reduce dopamine) might have a more glutamatergic condition instead
- Clozapine is an atypical antipsychotic that has better results with "treatment resistant" patients and this might be because it doesn't target dopamine (it targets serotonin instead)
7 |
Is the therapeutic potential of dopaminergic agents exhausted?
|
Should we give up on dopaminergic antipsychotics and start focusing on glutamates instead? Carlsson thinks there's still a future in dopamine research.
- Carlsson et al. are researching new drugs which regulate dopamine activity without producing harmful hypodopaminergia (which creates the unpleasant side-effects of antipsychotics)
- These work by acting at the pre-synapse (where dopamine is produced) rather than the post-synapse (where the dopamine receptors are), so they stop the brain producing too much dopamine without interfering with the brain's ability to process dopamine normally
- These drugs are "now in clinical trials" (and that was two decades ago!)
Conclusions
Carlsson suspects there are probably different groups of schizophrenia patients ("subpopulations") whose symptoms have different biological explanations - not always the Dopamine Hypothesis. There may be a subpopulation suffering from glutamatergic deficiency and these deserve "special attention".
Lack of glutamate might cause patients to have an exaggerated response to dopamine at the post-synapse. In other words, even though only normal levels of dopamine are being produced, the dopamine receptors have an extreme reaction.
Researchers should start looking into the role of other neurotransmitters, like gaba, acetylcholine and neuropeptides.
Carlsson suspects there are probably different groups of schizophrenia patients ("subpopulations") whose symptoms have different biological explanations - not always the Dopamine Hypothesis. There may be a subpopulation suffering from glutamatergic deficiency and these deserve "special attention".
Lack of glutamate might cause patients to have an exaggerated response to dopamine at the post-synapse. In other words, even though only normal levels of dopamine are being produced, the dopamine receptors have an extreme reaction.
Researchers should start looking into the role of other neurotransmitters, like gaba, acetylcholine and neuropeptides.

|
EVALUATING CARLSSON ET AL. AO3
|
|
EXEMPLAR ESSAY
|