

|
ETHICAL ISSUES IN PSYCHOLOGY
|
|
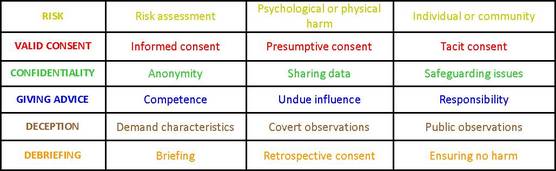
THE BPS CODE OF ETHICS (2014)
|

|
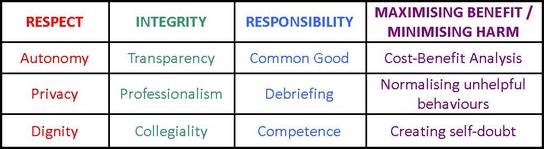
APPLYING ETHICAL ISSUES (AO2)
|

|
EVALUATING STUDIES ETHICALLY (AO3)
|

|
EXEMPLAR ESSAY
|