

|
WHAT ARE INDIVIDUAL DIFFERENCES IN MENTAL HEALTH?
Individual Differences refers to variables that make one person different from another.
Some individual differences appear in the features of schizophrenia and the features of depression which describe who is most at risk from these disorders. Psychometric tests like the Beck Depression Inventory (BDI) and Public Health Questionnaire (PHQ) are also measuring individual differences.
Because this is such a huge topic, I'll confine comments to schizophrenia and depression. You don't need to know all this information, just enough points (say, 4) to offer some evidence for individual differences affecting mental health.
CULTURAL DIFFERENCES
Schizophrenia
Schizophrenia seems to occur all over the world and affects about 1% of the population. However, Bhugra et al. (1999) found that it there are differences between Asian and Whites:
Black British people are more likely to suffer schizophrenia than any other ethnic group. This used to be blamed on migrants suffering stress and confusion in an unfamiliar culture, but the increased risk is still present in second generation Black British people. The British Institute of Psychiatry (2000) estimated Black people in the UK were 6 times more likely to develop schizophrenia than average. McCabe & Priebe (2004) compared different explanatory models of illness among people with schizophrenia from four cultural backgrounds: African-Caribbeans, West Africans, Bangladeshis and Whites. They found that Whites cited biological causes more than non-White groups, who were more likely to give supernatural or religious reasons.
Therefore it is possible that ethnic minority groups aren't really suffering more schizophrenia - they're just more likely to be diagnosed with it. This might be because of:
Unipolar Depression
Clinical depression is also a worldwide problem but affects from 2% to 19% in different countries. This suggests factors like poverty and exposure to violence play a role in the onset of depression. A cross-cultural study by Bromet et al. (2011) sampled 90,000 people in 18 countries. France and the USA were the most depressed and the poorer countries showed less rather than more depression. This supports the idea that depression is a disorder of Western nations, not just a psychological response to poverty, crime or war. 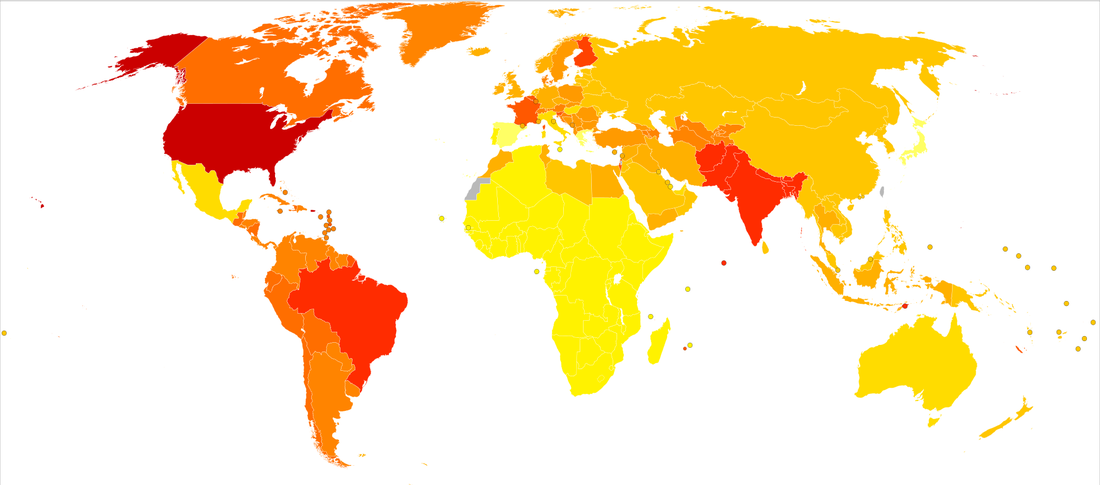
Worldwide prevalence of unipolar depression (2004): the darker red means more reported depression. This study shows the USA as the most depressed and Japan and Spain as the least - although India, Bangladesh and Pakistan are all in the top 5.
Geert Hofstede claims that individualist cultures are more prone to depression but collectivist cultures offer more support. This is backed up by a cross-cultural study by Chiao et al. (2009). Chiao suggests that people in Eastern countries have a greater genetic susceptibility to depression but have developed a collectivist culture as a way of reducing it; Westerners are less susceptible and have developed an individualistic culture, although this leaves them more at risk. This is using evolutionary psychology to explain culture and mental health.
However, India would usually be considered a collectivist culture and depression rates there are very high. Collectivist cultures put their own pressures on people to conform and feel shame and this can cause depression too. Another view would be that in collectivist cultures people are less willing to talk about depression, so it isn't diagnosed as often.
DEVELOPMENTAL DIFFERENCES
Schizophrenia
Schizophrenia may be classed as adolescent onset (10-17), early-adult onset (18-30), middle-age onset (30 -45) and late-onset (45+). The disorder does not suddenly “strike” and the obvious psychotic episode comes after less noticeable problems that might have existed for years. This makes it difficult to diagnose exactly when schizophrenia begins. The peak period of onset seems to be from 15-30. David Lewis (1996) claims children who later develop schizophrenia have 'premorbid' behavior (ie. unusual behaviour before they get ill) such as learning difficulties and behavioural problems. By age two, they are less likely to be walking and talking than other children. Lindmer et al. (2001) found that patients with late onset schizophrenia are more likely to be female, with less negative symptoms and have a shorter period of illness. Unipolar Depression
People are most likely to suffer their first depressive episode between 30-40 and there is a second, smaller peak of onset between 50-60. Depression can be an effect of dementia in the elderly. It can also be caused by loneliness and social isolation which can happen in old age. There is growing concern about depression in teenagers. Twenty years ago, depression in children was almost unknown. Now the fastest rate of increase in depression is among young people. There are several explanations for this:
These findings lend support to a Freudian view of depression, that it is a reaction to disturbed family relationships in early childhood - but that doesn't explain why the boys seem unaffected by the absent dads... although see below on why depression isn't diagnosed so much in males.
GENDER DIFFERENCES
Schizophrenia
Schizophrenia occurs equally in men and women. Kaplan et al. (1994) describe the peak ages of onset among men being between 15-25 years. The peak for women is 25-35 years but they also peak again in their 40s and 60s. Studies overwhelmingly support an earlier age of onset in males by 3-5 years, regardless of culture. Men tend to display more negative symptoms. Women tend to display less irrational thinking but more affective symptoms (emotional problems like depression, hostility, impulsivity and inappropriate behaviour). Szymanski et al. (1995) found women were diagnosed more frequently with disorganized subtypes of schizophrenia than men. Women were more likely to have delusions of persecution. Unipolar Depression
Population studies have consistently shown clinical depression to be about twice as common in women as in men (Bebbington, 1996), although it is unclear why this is so. There are several possible explanations:
As with cultural differences, it's also possible that women only appear to suffer this disorder more because they are more likely to be diagnosed with it. This is because in society it is more acceptable for women to talk about their feelings, which makes them more likely to present symptoms to a doctor. There is evidence that men express depressive feelings through drinking, aggression and work. Men are also more likely to commit suicide (Peter Orszag, 2015).
PERSONALITY DIFFERENCES
Schizophrenia
However, it's not clear whether this is explaining schizophrenia or just describing it. People with schizophrenia find it difficult to maintain social relationships and suffer mood swings so of course they score high for N and low for E.
Hans Eysenck also added P (psychoticism) to E and N to describe human personality. Psychoticism is "a halfway stage towards psychosis" (Heath & Martin, 1990). However, Eysenck uses P to describe criminals and psychopaths - and someone suffering a psychotic episode isn't necessarily one of those. Eysenck is probably confusing psychotic and psychopathic - easily done since they sound similar! 'Psychotic' means a break from reality but 'psychopathic' means an inability to feel compassion or empathy for other people. People with schizophrenia are still compassionate people and are NOT psychopaths!
Prospective longitudinal studies examine a cohort of people and monitor them over time to see if they develop a condition, then look for what they shared in common. De Graaf et al. (2002) followed 7076 Dutch adults for 12 months and those who developed mood disorders (including depression) had scored higher for N (neuroticism) than those who remained healthy. This suggests that personality traits (or at least N) might explain and predict depression rather than just describe it.
Unipolar Depression
High N (neuroticism) and low E (extroversion) are also linked to depression. However, as above, this may be just describing depression rather than explaining it: depressed people experience anxiety and they withdraw from social relationships, so of course they score high for N and low for E. Brown et al. (1985) identify self-esteem as an important personality trait that acts as a protection against the onset of depression during stressful life events. However, they also identify situational variables that are just as important for protecting against depression, such as social support.
|



|
OTHER DIFFERENCES: CULTURE-BOUND SYNDROMES
|
|
Culture-bound syndromes (or cultural disorders) are mental disorders which seem to affect a single cultural group. This means they are almost unknown outside of their own regions. They are sometimes called folk illnesses.
Faced with this baffling range of mental disorders around the world, psychologists used to think that it would be impossible to create a truly universal diagnostic system that could be applied internationally (like the ICD). However, Jane Murphy (1976) challenged this by demonstrating that many folk illnesses resembled Western mental disorders.
Murphy examined the Yorubas in Nigeria and a group of Inuit Eskimos in Alaska—groups that had no meaningful contact with modern culture. These tribes had names for disorders that appeared similar to schizophrenia, alcoholism and psychopathy. For example, the Inuit used the term “kunlangeta” to describe someone (usually a man) who lies, cheats and steals, is unfaithful to women and does not obey elders—very much like that of a Western psychopath. The Eskimos has a way of dealing with a person suffering from kunlangeta: “somebody would have pushed him off the ice when no one was looking.”
|
CULTURE-BOUND SYNDROMES FROM AROUND THE WORLD
|
However, not all cultural disorders "translate" into Western disorders this easily. There are some (like Mal de oro) which seem to mix symptoms from different conditions and others (like Amok ) which are in a category of their own.
|
For example, Koro is characterized by delusions of penis shrinkage; the sufferer panics and becomes convinced that when the penis vanishes, they will die. This idea makes sense in terms of Chinese culture, which emphasizes the healthy balance of "yin" and "yang" - masculine and feminine energies in the body and soul. Acts considered abnormal in Chinese culture (such as visiting prostitutes or masturbation) disturb the yin/yang balance.
|

|
In terms of Western medicine, this might be hypochondria or a psychotic episode, brought on by sexual shame, but it only makes sense for believers in Chinese philosophy.
Koro is also thought to be transmitted through food. In 1967, there was a koro epidemic in Singapore after newspapers reported cases of koro due to eating pork from a pig that had been given a drug against swine fever. Nearly 500 cases of koro were reported over 10 days.
Are there Western culture-bound syndromes? Anorexia nervosa has been suggested as a disorder which only affects people in Western cultures (but the study by Becker et al. argues it is learned from TV role models); Dissociative Identity Disorder (DID - multiple personality disorder) seems to affect only Americans and Europeans.
Koro is also thought to be transmitted through food. In 1967, there was a koro epidemic in Singapore after newspapers reported cases of koro due to eating pork from a pig that had been given a drug against swine fever. Nearly 500 cases of koro were reported over 10 days.
Are there Western culture-bound syndromes? Anorexia nervosa has been suggested as a disorder which only affects people in Western cultures (but the study by Becker et al. argues it is learned from TV role models); Dissociative Identity Disorder (DID - multiple personality disorder) seems to affect only Americans and Europeans.

|
APPLYING INDIVIDUAL DIFFERENCES TO MENTAL HEALTH
|

|
EVALUATING INDIVIDUAL DIFFERENCES IN MENTAL HEALTH (AO3)
|

|
EXEMPLAR ESSAY
|