

|
SYSTEMATIC DESENSITISATION
|
|
Counter-conditioning
This involves pairing the object, activity or creature that produces the fear response with something else that produces an incompatible response, like pleasure, relaxation or humour. Wolpe taught his patients relaxation techniques like controlling breathing. Larry Ventis uses humour therapy as a type of counter-conditioning (Ventis et al., 2001). |
Notice how Ventis helps Sarah learn new, harmless associations for spiders
|
The idea is that instead of their old Conditioned Response (CR) of fear, the patient learns a new CR, like relaxing or laughing.
|
Graduated Exposure
The therapist and the patient work out a STIMULATION HIERARCHY - a list of encounters with the feared thing, going from the least intense to the most intense. Less intense encounters tend to be:
|
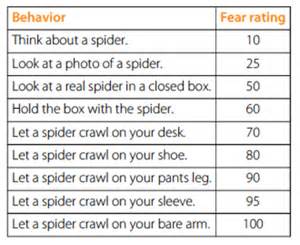
Example of a stimulation hierarchy for someone with a fear of spiders (arachnophobia)
|
It's very important that the stimulation hierarchy is created by the patient not the therapist. This is for two reasons:
- The patient knows best what makes them anxious. Having control over how the therapy proceeds is itself relaxing.
- It would be unethical to expose patients to distressing situations if they hadn't given informed consent to every step in the process first. Ethical guidelines emphasise the importance of respecting people's autonomy (control over what happens to them)
|
During systematic desensitisation, the patient works their way through the stimulation hierarchy, starting with the least intense encounters and building up to the most intense.
|
Drew uses systematic desensitisation to overcome a fear of heights (acrophobia)
|
Participant Modelling
Systematic desensitisation is based on classical condition, but Social Learning Theory can also be used to improve the therapy.
Douglas Bernstein (1979) calls this participant modelling. A first step on the stimulation hieraarchy would be to watch someone else model the relaxation techniques and encounter the feared object before trying it yourself.
With really severe phobias, the patient can't even bear to watch someone else encounter the feared object. In these cases Richard Sharf (2000) recommends covert modelling. This is where the first step on the stimulation hierarchy is to imagine someone else encountering the feared object.
Systematic desensitisation is based on classical condition, but Social Learning Theory can also be used to improve the therapy.
Douglas Bernstein (1979) calls this participant modelling. A first step on the stimulation hieraarchy would be to watch someone else model the relaxation techniques and encounter the feared object before trying it yourself.
With really severe phobias, the patient can't even bear to watch someone else encounter the feared object. In these cases Richard Sharf (2000) recommends covert modelling. This is where the first step on the stimulation hierarchy is to imagine someone else encountering the feared object.

|
SYSTEMATIC DESENSITISATION
|
|
This is because it's hard to re-create these things in the therapy session and hard to manipulate these things into a stimulus hierarchy. With a fear of flying (aerophobia), you're either flying or you're not. The sufferer isn't frightened of aeroplanes or films set on aeroplanes; it's actually being up in the air themselves that they find frightening.
In the past, in vitro techniques involved the patient imagining themselves to be in the frightening situation. These days, virtual reality is helping to apply systematic desensitisation to situations that used to be difficult to set up in a therapy session. |
I want to play "Skyrim" this way
|
DIFFERENCES
Systematic desensitisation involves gradual exposure to the object you fear, but with flooding you are completely exposed to it, all at once. It's like going directly to the end of the stimulus hierarchy and skipping all the stages in between.
Systematic desensitisation is much more ethical than flooding, because the participants are only exposed gradually to the thing that they fear and they only move on to greater exposure when they feel ready. With flooding, the patient is exposed to the object they fear all at once, in a very intense way. This can be distressing.
Both therapies can be carried out in vitro rather than in vivo. Imagining exposure to the feared object is less distressing. However, in vitro flooding is still more upsetting that in vitro systematic desensitisation.
Neither systematic desensitisation nor flooding tackle the possible underlying problem behind the phobia. They are both behavioural therapies that only deal with the symptoms, not the cause. If there is an underlying problem behind the phobia (like trauma in the patient's past), then that will still be there and will carry on causing difficulties, even if the phobia is temporarily eased.
Systematic desensitisation is much more ethical than flooding, because the participants are only exposed gradually to the thing that they fear and they only move on to greater exposure when they feel ready. With flooding, the patient is exposed to the object they fear all at once, in a very intense way. This can be distressing.
Both therapies can be carried out in vitro rather than in vivo. Imagining exposure to the feared object is less distressing. However, in vitro flooding is still more upsetting that in vitro systematic desensitisation.
Neither systematic desensitisation nor flooding tackle the possible underlying problem behind the phobia. They are both behavioural therapies that only deal with the symptoms, not the cause. If there is an underlying problem behind the phobia (like trauma in the patient's past), then that will still be there and will carry on causing difficulties, even if the phobia is temporarily eased.
APPLICATIONS
Rothbaum et al. (1995) created a virtual-reality helmet worn by the patient which displays a phobic situation which is controlled by the therapist. The scene might be one of driving a car over a high bridge. The pulse rate is monitored by the therapist. When the pulse rate gets too high, the scene is frozen in frame. The therapist then uses counter-conditioning to replace the fear with relaxation techniques.
This sort of technology is replacing in vitro therapy, making systematic desensitisation more ethical without losing its effectiveness; it also enables systematic desensitisation to be applied to phobias of things other than animals or objects.
This sort of technology is replacing in vitro therapy, making systematic desensitisation more ethical without losing its effectiveness; it also enables systematic desensitisation to be applied to phobias of things other than animals or objects.