

|
PSYCHOLOGICAL TREATMENTS FOR DEPRESSION
The Unit 2 Exam expects you to know about one psychological treatment for a disorder other than schizophrenia; here, unipolar depression and cognitive therapy.
You are also expected to understand a non-biological explanation of depression which is linked to this treatment. There are other psychological treatments besides CBT. For example, there is psychoanalysis (Freud's "talking cure") and behavioural therapy (like token economy programmes) but these are less commonly used and more controversial.
Some students who enjoyed Freud in Unit 1 might prefer to write about Freud's psychoanalysis as a psychological treatment for depression. I've included some sections on this that other students may ignore.
|
|
DEPRESSION & COGNITIVE BEHAVIOURAL THERAPY (CBT)
|
|
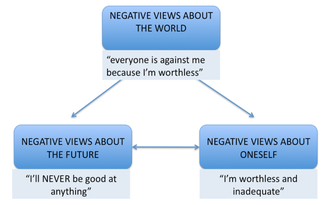
Beck proposed the Cognitive Triad. This is the idea that our thoughts and beliefs shape our feelings and our feelings then direct the way we behave; our behaviour then influences the way other people treat us and that in turn backs up our thoughts and beliefs.
Beck suggests a lot of behavioural problems stem from "faulty thinking" - core beliefs that are negative and irrational. For example, if a person thinks that people don't like them, they will feel bitter and upset. If they feel this way, they will act defensively and be aloof and cold. If they behave this way, people won't like them... |

The Cognitive Triad is an example of a VICIOUS CIRCLE. Beck's therapy was an attempt to re-wind the negative process and create a 'virtuous circle'.
|
|
Beck's cognitive therapy was a gentle process, getting clients to question their core beliefs. Albert Ellis' Rational Emotive Behavioural Therapy (REBT) was more aggressive. Ellis believed faulty thinking should be challenged and exposed for what it was.
Ellis proposed the A-B-C Model of behavioural change: |

|
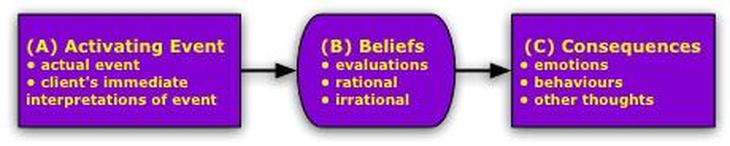
The therapist gets the client to identify an "activating event" - something they believe is the trigger for their problems. For someone with unipolar depression, this might be a stressor like work, family conflicts or social interactions. The client then identifies their "beliefs" about this event. People with depression often think that other people are critical of them or that tasks are beyond their ability. Therapist and client then explore the "consequences" of these beliefs, such as how socially withdrawing from people or challenges leads to isolation and failure.
|
Ellis also proposed a fourth step - D for "dispute" - in which the therapist challenges the client's beliefs, exposes them as faulty and gets the client to adopt different beliefs (for example, that other people are not judging you or that tasks can be accomplished).
It's important that the "D" part is non-judgmental. The therapist isn't trying to make the client feel bad for having these beliefs.
|
|
|
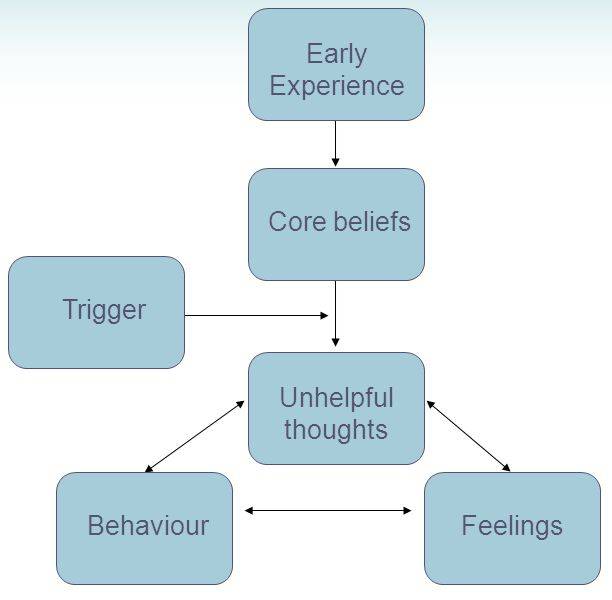
Cognitive Behavioural Therapy (CBT) combines Beck's and Ellis' therapies. A CBT therapist encourages the client to become aware of their own core beliefs, which may have been formed by unpleasant early experiences.
They then work out what sort of events act as triggers for unhelpful thoughts. Therapist and client decide decide how to put these beliefs to the test, perhaps through role-playing what happens when they act on their unhelpful thoughts compared to when they act on more positive thoughts. |
Kendall & Hammen (1998) summed up 4 basic assumptions in CBT like this:
- Patients’ interpretations of themselves and the world around them are different from what is actually the case.
- Thoughts, behaviour and feelings are interrelated and so it is wrong to identify one of these factors (eg. behaviour) as being more important than the others.
- Treatment needs to change the way people think about themselves and the world around them.
- Treatment needs to change the client’s cognitive processes and behaviour; the benefits will be greater by tackling both.
3-minute video summing up CBT
WHAT ABOUT PSYCHOANALYSIS?
Psychoanalysis is the original "talking cure" that inspired Aaron Beck. It also involves one-to-one session with a therapist (called a psychoanalyst).
Unlike CBT, psychoanalysis focuses on unconscious feelings and desires. Because the client cannot know their own unconscious mind, there's no point in the sort of activities that CBT involves. Instead, the analyst has to help the client understand his or her unconscious. This is done through activities like dream analysis, free association or the Rorschach inkblot test.
The assumption in psychoanalysis is that the client's problems stem from childhood trauma - probably a traumatic relationship with a parent. There may be memories of childhood abuse that the client has repressed. The client's depression is in fact a defence mechanism to avoid facing these memories. The traumatic memories must be brought into the conscious mind and confronted so that the defence mechanisms are no longer needed.
Unlike CBT, psychoanalysis focuses on unconscious feelings and desires. Because the client cannot know their own unconscious mind, there's no point in the sort of activities that CBT involves. Instead, the analyst has to help the client understand his or her unconscious. This is done through activities like dream analysis, free association or the Rorschach inkblot test.
The assumption in psychoanalysis is that the client's problems stem from childhood trauma - probably a traumatic relationship with a parent. There may be memories of childhood abuse that the client has repressed. The client's depression is in fact a defence mechanism to avoid facing these memories. The traumatic memories must be brought into the conscious mind and confronted so that the defence mechanisms are no longer needed.

|
APPLYING PSYCHOLOGICAL TREATMENTS FOR DEPRESSION
|
|
Following Beck’s approach, the therapist helps the client identify negative thoughts in relation to themselves, their world and their future, using Beck’s negative triad.
The client and therapist work together to investigate these irrational thoughts, discussing evidence for and against them. |
|
Ellis' REBT
Like Beck's approach, REBT challenges irrational thoughts. However, Ellis’s theory does this through dispute (argument). The therapist will dispute the client’s irrational beliefs, trying to replace them with reasonable beliefs. There are different types of disputing styles:
- logical dispute: the therapist questions the logic of irrational thoughts ("why would your friends not want you to go to the cinema with them?")
- empirical dispute: the therapists asks for evidence for irrational thoughts ("what evidence do you have that they don't want to see you?")
For Beck, the warm personal relationship between therapist and client is essential. In Beck's therapy, the therapist is helping the client discover things for themselves. Ellis views the therapist as a teacher and• REBT is more about persuasion and confrontation.
Both types of CBT set the client homework, which involves putting these negative/irrational thoughts to the test (eg asking a friend to come over for coffee to see if they refuse)
3-minute video showing CBT in action
APPLYING & EVALUATING PSYCHOANALYSIS
Psychoanalysis tries to uncover the depressed person’s repressed memories and allow them to gain insight into the cause of their depression. There are several techniques for this:
- Free association: the client says whatever comes into his or her mind and the analyst looks for connections between seemingly-unconnected ideas. According to Freud, long pauses indicate that the client is uncovering repressed ideas. Techniques like the Rorschach inkblot test can help with free association.
- Dream analysis: in dreams the "censor" in our minds that keeps the repressed thoughts in the unconscious is less effective. Repressed material in dreams appears in disguised or symbolic form. Dream analysis involves interpreting the symbol and questioning clients about their dreams to work out what they mean.
- Transference: The client transfers feelings they have towards their parents onto the analyst. Transference brings to the surface conflicts from the client's childhood and uncovers repressed memories.
Unlike CBT, psychoanalysis is a global therapy. It is trying to bring the client's entire life into balance, not just fix a few symptoms and dysfunctional behaviours. If it is successful, it brings about a personal transformation.
Unlike CBT, the psychoanalyst is neutral. In fact, sessions can happen where the analyst doesn't speak at all!
Shapiro & Emde (1991) criticise psychoanalysis for depression. Psychoanalysis requires the client to be very motivated and engaged - exactly what people with depression are not. In CBT (especially Ellis' REBT) , the therapist takes charge and is more directive and this might be what clients with depression need.
Psychoanalysis also takes a long time - possibly years. People with severe depression need a quicker cure, especially if they are at risk of harming themselves
Shapiro & Emde (1991) criticise psychoanalysis for depression. Psychoanalysis requires the client to be very motivated and engaged - exactly what people with depression are not. In CBT (especially Ellis' REBT) , the therapist takes charge and is more directive and this might be what clients with depression need.
Psychoanalysis also takes a long time - possibly years. People with severe depression need a quicker cure, especially if they are at risk of harming themselves
However, modern psychoanalysis has taken on some of the techniques from CBT to be more directive and less leisurely; these sort of sessions take place 5 times a week for 6 months. Falk Leichsenring (2001) carried out a meta-analysis to compare modern psychoanalysis and CBT and found them equally effective in 58 out of 60 cases.
Crash Course Psychology looks at psychotherapy of all sorts: psychoanalysis is at 1:30 and cognitive therapy is at 8:20
|
EVALUATING PSYCHOLOGICAL TREATMENTS
|
|
This is a crazy study! Zindel Segal takes people who had recovered from depression, makes them sad again then waits to see if they get depressed all over again - and they do! Nice work, psychology!
I should also point out that 127 patients finished their treatment, 99 of them went through "sadness provocation" but only 79 were tested 18 months later, so there's a huge drop-out rate there. Sample attrition is something lots of these prospective studies into depression suffer from. |
Here's the music Segal used. Listen to it and think of the saddest experience you've had. Sorry, I couldn't find a version of it at half speed.
(and yes, the position of the Youtube play button makes this guy look a bit like Hitler...) |
Hollon et al. (2005) studied patients who received treatment for 16 weeks then were observed for 12 months to see if their symptoms returned (relapse). There were 3 groups: (1) patients who received CBT; (2) patients who received drug therapy; and (3) patients received drug therapy which continued over the 12 month observation period. Only 31% of CBT patients suffered a relapse compared to 76% of those treated with drugs and 47% of the patients who carried on taking antidepressants.
These findings suggest that drug therapy is only palliative whereas cognitive therapy offers a better cure.
The NHS recommends an "integrated approach" involves combining the two treatments. Antidepressants might give some patients the confidence and concentration to take part in CBT. It may be possible to reduce the dependency on antidepressants as the cognitive therapy takes effect.
These findings suggest that drug therapy is only palliative whereas cognitive therapy offers a better cure.
The NHS recommends an "integrated approach" involves combining the two treatments. Antidepressants might give some patients the confidence and concentration to take part in CBT. It may be possible to reduce the dependency on antidepressants as the cognitive therapy takes effect.
Applications
The National Institute for Clinical Excellence (NICE) recommends CBT as the first liner of treatment for mild to moderate depression. Since NICE and the NHS are government-funded, this represents government backing for CBT in the UK.
CBT is free on the NHS, but there are waiting lists. If you pay for private therapy, CBT may cost £40-100 per session. That sounds like a lot, but it's cheaper than psychoanalysis.
CBT is free on the NHS, but there are waiting lists. If you pay for private therapy, CBT may cost £40-100 per session. That sounds like a lot, but it's cheaper than psychoanalysis.
Starting in 2008, the Increasing Access to Psychological Therapies (IAPT) programme is a project to extend psychotherapy like CBT and psychoanalysis to more people who need it in the UK. Nearly 900,000 people a year use these services now and the programme aims to extend this to 1.5 million by 2021.

|
EXEMPLAR ESSAY
|