

|
HOW CAN WE TREAT PHOBIAS?
A phobia is an irrational fear of something other people think is harmless. Because it's an irrational fear, sufferers will be terrified of just the sight or even the mention of the feared thing, even though they know it doesn't pose any danger. Most phobics know that their fear is irrational, but they feel it anyway.
You might think "Surely everyone's frightened of death!" but an irrational fear of death makes you terrified of graveyards, going to funerals or watching news items where someone has died
Phobias can be very debilitating because they stop people living normal lives. Agoraphobics can't bring themselves to go outside and aerophobics can't take holidays that involve flying.
Whether airlines should offer passengers treatment for the fear of flying (aerophobia) is a popular Key Question for the Learning approach. There's a Blog entry on it here.
How you treat a phobia depends on what you think is causing it:
In the real world, these therapies are often combined. For example, cognitive therapy and behavioural therapy work well together and form Cognitive-Behavioural Therapy (CBT). This therapy seems to combine behavioural treatment with cognitive therapy (tackling Marvin's memories and emotions at the same time)
For this course, you need to know about two behavioural therapies; one of them has to be systematic desensitisation and I'm offering flooding as the other. PHOBIAS AS BEHAVIOURAL PROBLEMSThe Learning Approach views phobias as behavioural problems. This means they are a type of unpleasant behaviour - like a bad habit. The feelings of fear and stress are caused by the behaviour, rather than the other way round. If people could act in a calm way around their feared object, they would feel a lot calmer too.
This is counter-intuitive. We normally think of fearful behaviours being caused by feelings of terror, rather than feelings of terror being produced by fearful behaviours. But just because an idea goes against what we expect, it doesn't make it wrong.
So where do these behavioural problems come from? According to the Learning Approach we are not born with them - we are born as a "blank slate" (tabula rasa) and we learn things like phobias from experience.
The phobia begins with an Initial Sensitising Event (ISE), some sort of distressing or traumatic moment that triggered the fearful behaviour in the first place. This is explained with classical conditioning: 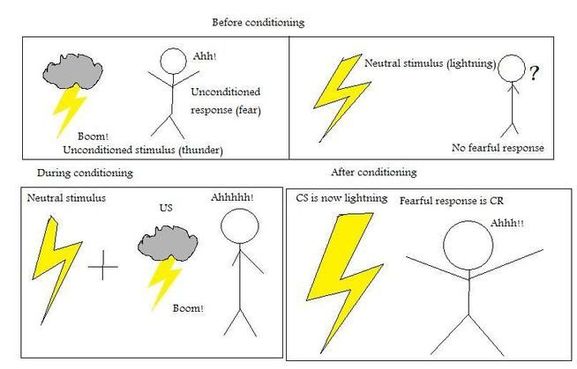
Most phobias are learned in early childhood, because babies have strong fear-responses and don't know enough about the world to realise what is really frightening them. You can see a phobia being acquired by a baby in the Classic Study by Watson & Rayner (1920).
Once the phobia is in place, other sorts of conditioning might keep it going or make it more intense:
Operant conditioning might reinforce the phobia, because panicking might attract attention and concern from other people or just make the feared thing go away. 
Eek! A mouse! This old-fashioned (and sexist) stereotype of female phobia is explained on TV Tropes, which links the phobia to evolutionary psychology
Social Learning Theory explains how people might see role models reacting to feared objects with great panic and imitate that reaction.

Evil clowns in the media might explain the rise of the fear of clowns (coulrophobia) - this news article looks at the history of frightening clowns
|


|
BEHAVIOURAL THERAPIES
|
|
A related problem is that behavioural therapies ignore cognitions. Cognitions include the feelings of fear that make up the phobia and if you ignore this you are missing out on the emotional side of the phobia and what it is about the feared object that the sufferer finds so distressing. Sometimes phobia-sufferers have false beliefs about the object of their fear (for example, aerophobes usually exaggerate the risks of flying in their own minds). These false beliefs can and should be challenged and re-educated, but behavioural therapies don't do this.
|
... it's still the safest way to travel
|
DIFFERENCES
The similarities that all behavioural therapies share in common have been discussed above. The differences will be discussed on the particular pages for systematic desensitisation and flooding.
A different sort of therapy focuses on the feelings of fear rather than the fearful behaviours. Cognitive therapy and psychoanalysis are examples of this.
Cognitive Therapy encourages the sufferer to understand that their phobia is irrational. This sort of therapy helps the sufferer to look at the feared object differently, perhaps see it in a more positive light, and develop coping strategies to overcome the anxiety and stress. This may involve working out what the ISE was and helping the sufferer to "put it in the past".
Psychoanalysis goes deeper than this, looking for the original cause of the phobia, which is usually a childhood trauma. One of Freud's patients, a boy called Little Hans, had a phobia of horses. Freud concluded the boy was really in fear of his father and the fear of horses was a defence mechanism.
So both of these therapies go back to investigate the ISE that "triggered" the phobia in the first place and offer ways of undoing the original problem.
In contrast, behavioural therapies like systematic desensitisation and flooding aren't very interested in what the ISE was. They focus on fixing the phobia as it is today, not how it started in the past. These therapists believe that, if sufferers can change their behaviour, the feelings of fear will fade of their own accord.
A different sort of therapy focuses on the feelings of fear rather than the fearful behaviours. Cognitive therapy and psychoanalysis are examples of this.
Cognitive Therapy encourages the sufferer to understand that their phobia is irrational. This sort of therapy helps the sufferer to look at the feared object differently, perhaps see it in a more positive light, and develop coping strategies to overcome the anxiety and stress. This may involve working out what the ISE was and helping the sufferer to "put it in the past".
Psychoanalysis goes deeper than this, looking for the original cause of the phobia, which is usually a childhood trauma. One of Freud's patients, a boy called Little Hans, had a phobia of horses. Freud concluded the boy was really in fear of his father and the fear of horses was a defence mechanism.
So both of these therapies go back to investigate the ISE that "triggered" the phobia in the first place and offer ways of undoing the original problem.
In contrast, behavioural therapies like systematic desensitisation and flooding aren't very interested in what the ISE was. They focus on fixing the phobia as it is today, not how it started in the past. These therapists believe that, if sufferers can change their behaviour, the feelings of fear will fade of their own accord.
APPLICATIONS
|
The applications of systematic desensitisation and flooding are discussed on their particular pages.
The latest virtual reality techniques help phobia-sufferers experience the situations that frighten them while knowing they are completely safe. This helps them practise coping techniques like relaxation before they encounter the real thing later in the therapy. This is a big improvement on in vitro therapies. |
|